


Key Takeaways

User Profile
Hello Heart Hero.
You may be here because your watch buzzed with an irregular rhythm alert, or because you felt a flutter in your chest and then heard a confusing phrase in clinic: lone atrial fibrillation. That combination can leave anyone unsettled. You feel something real in your body, but the explanation sounds vague, almost dismissive.
If you've also felt skeptical about the healthcare system, that's understandable. Many people leave appointments with more questions than answers, especially when a rhythm problem comes and goes. It can feel like you're expected to trust a label without really knowing what it means, why it happened, or what you're supposed to do next.
Lone atrial fibrillation is a term with a long history, and it still matters. But the meaning has shifted as heart imaging, rhythm monitoring, and wearable devices have improved. So if you're trying to make sense of your symptoms through your Apple Watch, Fitbit, Kardia, or Samsung device, you need a modern explanation, not an outdated one.
Your Guide to Understanding Lone Atrial Fibrillation
Atrial fibrillation, often shortened to AFib, is a rhythm problem that starts in the heart's upper chambers, called the atria. Instead of sending out one organized electrical signal, the atria fire in a scattered way. The result is a heartbeat that can feel chaotic, jumpy, fast, or simply “off.”
The word lone was historically used when AFib showed up in someone without obvious structural heart disease or the usual major heart-related conditions doctors often associate with AFib. In older medical descriptions, this often meant a younger, otherwise healthy person whose tests didn't show the common explanations.
That history is real. In a classic Circulation cohort, patients with lone AF were predominantly male at 78% and had a mean age of 44.2 years at diagnosis according to Circulation. That helped create the classic image of lone atrial fibrillation as AFib in a younger, structurally normal heart.
Why this diagnosis can feel confusing
The confusion comes from the fact that “lone” does not mean “nothing is going on.” It means doctors haven't found the usual larger, more obvious causes.
That distinction matters a lot. A normal basic workup doesn't always rule out subtle electrical changes, early atrial changes, or patterns that only show up over time.
Lone atrial fibrillation is best understood as AFib without the usual obvious heart disease, not AFib without any possible underlying reason.
Why your wearable matters
For many people, episodes happen at home, during sleep, after stress, after alcohol, or during a random quiet moment on the couch. That's one reason wearables are changing this conversation. They let you catch rhythm changes when no clinic monitor is attached and no one else is watching.
Used well, a wearable doesn't replace a clinician. It gives you a clearer record of what your heart is doing so your next conversation can be based on evidence, not guesswork.
What Exactly Is Lone Atrial Fibrillation
To understand lone atrial fibrillation, it helps to first understand ordinary atrial fibrillation in plain language.
Your heart runs on electricity. In a steady rhythm, the signal starts in the right place, moves in an orderly path, and tells the heart muscle when to squeeze. This process is similar to a drummer keeping a band on time. When the beat is steady, everyone stays coordinated.
With AFib, that steady beat gets scrambled. The upper chambers start firing off disorganized signals, and the lower chambers receive an irregular pattern. That can create a pulse that feels uneven and unpredictable.
What the word lone was meant to capture
Doctors used the term lone atrial fibrillation for people, often younger adults, who had AFib without the more familiar findings such as obvious structural heart disease. It was a way of saying, “this is AFib, but not the usual kind we see in older patients with several heart conditions.”
Simple definition: Lone atrial fibrillation traditionally meant AFib in a person under 60 without overt structural heart disease or major associated illness.
A good analogy is a house with a flickering light switch. If the wiring panel looks normal and the walls look intact, the flicker still happened. You just haven't found a big visible cause yet. That is how lone AF was often approached.
If you want a broader overview of rhythm problems in general, this guide on heart rhythm disorders can help place AFib in context.
The classic profile, and why it still matters
Historically, lone AF had a recognizable pattern. Patients were often younger and otherwise healthy on basic evaluation. The older studies helped clinicians separate these patients from people whose AFib was tied to heart failure, coronary disease, valve disease, or longstanding high blood pressure.
That doesn't mean everyone with lone AF fits a stereotype. It means the term came from a pattern doctors saw again and again.
Why the term can mislead patients
Many people hear “lone” and assume it means harmless. That's where trouble starts.
The label was never supposed to mean “ignore this.” It was supposed to describe a subgroup. Even in that subgroup, the rhythm itself is still real, symptoms still matter, and follow-up is still important.
How Lone AF Differs From Other Types of AFib
Some AFib develops in a heart that already shows clear stress or damage. Common examples include AFib that appears alongside long-term high blood pressure, heart failure, valve disease, or other structural heart changes. In those cases, the rhythm problem is part of a larger picture.
Lone atrial fibrillation was different because it referred to AFib without those obvious structural findings. That difference shaped how doctors thought about risk, prognosis, and treatment.
The old idea versus the modern view
The old view was fairly simple. If a younger person had AFib and standard testing didn't show heart disease, the episode might be called lone AF.
The modern view is more careful.
Expert reviews note that even in patients labeled as lone AF, there can be measurable atrial mechanical impairment and subtle ECG changes, which suggests the term doesn't guarantee a completely normal atrium beneath the surface, as summarized in this systematic review on lone AF.
That means your heart can look “normal” on a basic check while still showing small-scale electrical or mechanical changes that matter.
Why the label is used less casually now
As testing improved, doctors started finding issues that older evaluations could miss. Better echocardiograms, longer rhythm monitoring, and more refined definitions have narrowed who fits the lone AF category.
If you'd like a simple explanation of the kinds of conditions doctors are trying to rule out, this overview of structural heart disease is useful.
A modern diagnosis is often less about proving your heart is perfect and more about carefully excluding the major conditions that change treatment and long-term risk.
A comparison that helps
Here is the practical difference many patients want to know:
- AFib with structural heart disease often has a visible partner problem. The heart muscle, valves, or chambers show a reason to be concerned.
- Lone atrial fibrillation historically meant AFib without that visible partner problem on routine evaluation.
- Modern “lone” AF is a narrower category because doctors now recognize that subtle atrial abnormalities may still be present.
So if you're thinking, “If my heart is healthy, why am I having this?”, the honest answer is that “healthy” can mean different things depending on how thoroughly the heart has been evaluated.
Symptoms and Modern Diagnosis with Wearables
For many people, lone atrial fibrillation doesn't begin with a diagnosis. It begins with a moment.
You feel pounding in your chest while folding laundry. Your watch says your pulse is irregular while you're lying in bed. You stand up, feel breathless, then ten minutes later everything seems normal again. By the time you try to explain it, the episode is over.
That stop-and-start nature is one reason AFib can be frustrating.
What symptoms can feel like
Symptoms vary a lot. Some people feel every beat. Others barely notice anything.
Common experiences include:
- Palpitations that feel like fluttering, racing, skipping, or a fish flopping in the chest
- Shortness of breath during activities that usually feel easy
- Fatigue that seems out of proportion to what you're doing
- Lightheadedness or a vague shaky feeling
- Chest discomfort or pressure, though that should always be taken seriously
Some people have no symptoms at all and only find out because of a wearable alert.
Why wearables changed the game
Wearable ECGs and rhythm notifications have made it easier to catch fleeting episodes. That matters because lone AF has become harder to define casually as technology improves. Reviews note that its estimated prevalence has fallen from about 30% in early studies to about 3% in the Euro Heart Survey, reflecting how better diagnostics reclassify many cases once thought to be lone AF, according to Europace.
In plain language, newer tools are exposing details that older tools missed.
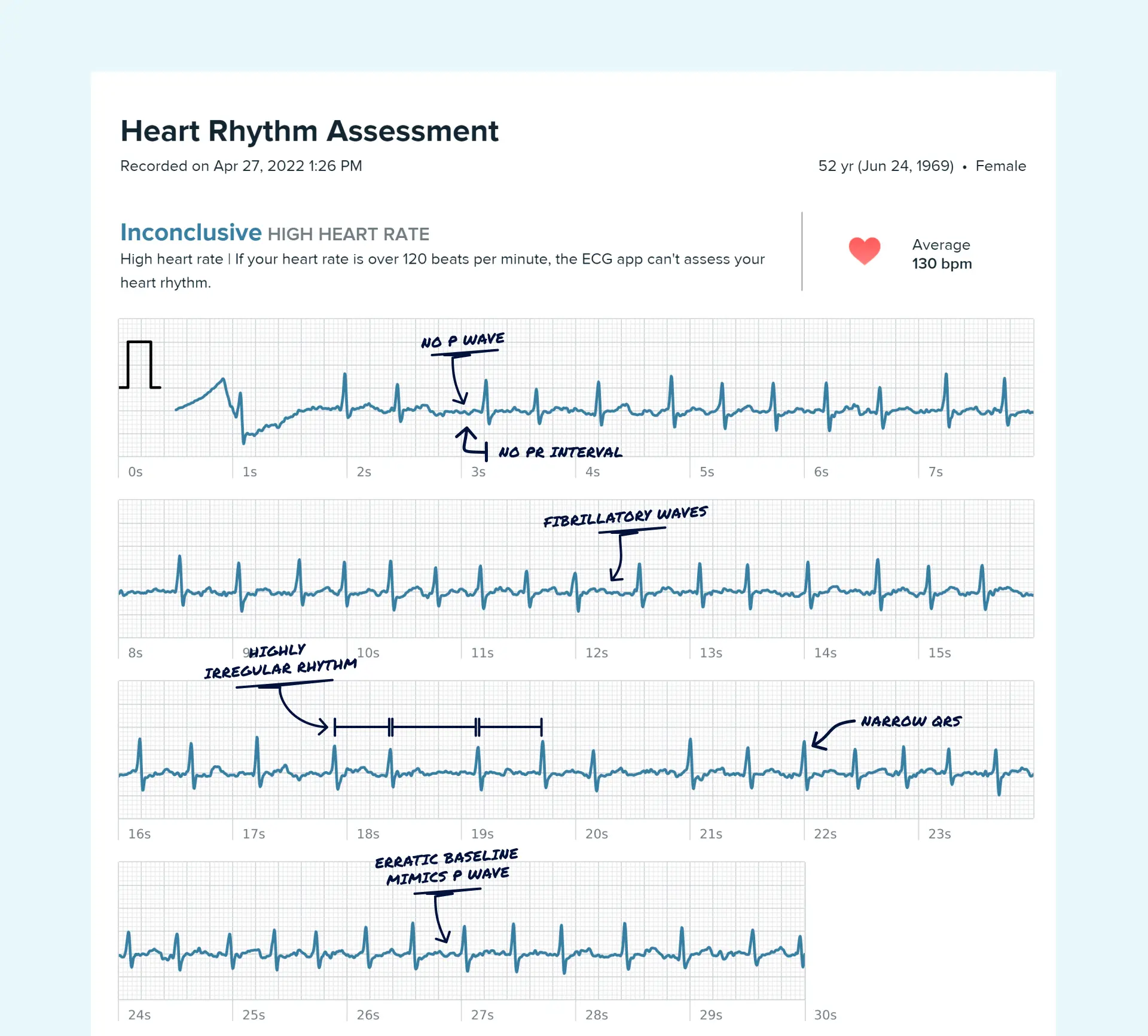
If you're using a smartwatch or handheld ECG, learning what AFib can look like on those tracings is helpful. This visual guide to what AFib looks like on your watch ECG can make those recordings less mysterious.
What to capture when an episode happens
A wearable is most useful when you gather context, not just a screenshot.
Try to note:
- When it started and how long it lasted
- What you were doing right before it happened
- How you felt during the episode
- Whether the rhythm looked irregular again later the same day or week
Practical rule: A single alert can start the conversation, but a pattern over time helps doctors make a modern diagnosis.
That pattern is especially helpful when symptoms come and go and your clinic ECG is normal.
Understanding Your Health Risks and Prognosis
This is often the hardest part to talk about, because the word stroke can overwhelm everything else.
It's important to stay grounded. Lone atrial fibrillation was once viewed as relatively benign compared with AFib in older patients with multiple conditions. But “lower risk” is not the same as “no risk.”
A 2022 study of lone AF patients found that over 5.8 years of follow-up, stroke occurred in 10% of patients and 12% progressed from paroxysmal to permanent AF, according to this 2022 lone AF cohort study. That tells us two things. First, lone AF deserves follow-up. Second, risk can change over time.




Why doctors talk about stroke risk even when you're younger
AFib can allow blood to move less efficiently through part of the atrium. When blood lingers, clots can form more easily. If a clot travels to the brain, it can cause a stroke.
That doesn't mean this will happen to you. It means your clinician is trying to estimate risk before a bad event occurs.
One tool doctors often use is the CHA2DS2-VASc score. You don't need to memorize the letters. What matters is the idea behind it. Your doctor is looking for conditions and personal factors that make clot risk higher, such as age and other medical history.
Why blood thinners may still come up
Patients sometimes feel offended or frightened when anticoagulation enters the conversation. “Why would I need that if this is lone AF?” is a fair question.
The answer is that treatment decisions aren't based on the word lone by itself. They're based on your total risk picture, your age, your episode pattern, and what else becomes apparent over time.
A few practical truths help:
- Rhythm type matters. Short, occasional episodes raise different questions than ongoing or increasingly frequent AFib.
- Your risk profile matters more than the label. A lone AF diagnosis in the past doesn't freeze your risk forever.
- Prevention is the goal. Doctors would rather prevent a stroke than react to one.
What prognosis often depends on
For many people, prognosis depends less on the name and more on a cluster of real-world details:
- symptom burden
- how often episodes happen
- whether they are getting longer
- what follow-up testing shows
- whether other conditions appear later
If you're tracking episodes with a wearable, it can also help to understand your AFib burden, which is the broader pattern of how much AFib is occurring over time.
The most reassuring approach is not denial. It's steady monitoring, honest follow-up, and early action when patterns change.
Lifestyle and Management Strategies for Lone AF
Once the fear settles a bit, many individuals ask the most useful question: “What can I do?”
Many factors play a role. Not everything is under your control, but many people do notice patterns, triggers, and habits that affect how often episodes happen or how intense they feel.
The two main treatment mindsets
Doctors often talk about rate control and rhythm control.
- Rate control means letting AFib occur but slowing the heart rate so the body tolerates it better.
- Rhythm control means trying to keep the heart in normal rhythm or restore it when AFib occurs.
Those sound technical, but the difference is simple. One strategy calms the speed. The other tries to change the rhythm itself.
Daily habits that often matter
These changes aren't glamorous, but they can be powerful:
- Sleep matters more than many people realize. Poor sleep can make the heart more irritable.
- Alcohol can be a trigger. Some people notice symptoms after even modest intake.
- Stress can shape the body's electrical environment. The heart and nervous system are closely linked.
- Caffeine is individual. Some tolerate it well. Others notice a clear connection.
- Hydration and steady routines help some people feel less vulnerable to sudden episodes.
A simple symptom and trigger log can teach you more than guessing ever will.
Food and exercise without extremes
You do not need a perfect diet. You need a sustainable one.
Many patients prefer a heart-healthy eating pattern that reduces highly processed foods and builds meals around vegetables, legumes, fish, olive oil, nuts, and whole grains. If you want help putting that into daily practice, a Mediterranean diet AI meal planner can be a practical way to turn a broad idea into actual meals.
Exercise usually helps overall heart health, but extremes can muddy the picture. Moderate, consistent activity is often easier on the body than a cycle of total inactivity followed by intense weekend efforts.
Your goal isn't to become fragile. It's to make your internal environment more predictable.
What management looks like in real life
Good management often combines several layers:
- Track symptoms and rhythm episodes
- Reduce personal triggers where possible
- Follow up when the pattern changes
- Review treatment options if symptoms affect daily life
That approach gives you more agency and helps you show up to appointments with useful information instead of just worry.
How to Partner with Your Doctor Using Qaly
The strongest position you can be in is not “I know more than my doctor” or “I should just trust everything blindly.” It's partnership.
That partnership works best when you bring organized evidence. A vague memory of “my heart felt weird a few times last month” is hard for any clinician to act on. A set of dated wearable ECGs, symptom notes, and trend observations is much more useful.
What good preparation looks like
Before an appointment, it helps to gather:
- Your rhythm recordings from devices like Apple Watch, Fitbit, Kardia, Samsung, or Withings
- A short symptom timeline with dates, times, and what you were doing
- Questions you don't want to forget, especially about stroke risk, episode pattern, and treatment options
This changes the tone of the visit. Instead of trying to reconstruct a stressful episode from memory, you're discussing actual data.
Where Qaly fits
One option some wearable users use is Qaly. It lets people upload at-home and wearable ECGs for human-reviewed interpretation, track interval and rhythm trends over time, and generate reports they can share with healthcare professionals.
That can be especially helpful if your episodes are brief, happen outside office hours, or keep leaving you with uncertain smartwatch readings. It doesn't replace your doctor, and it shouldn't. It gives you cleaner information to bring into the relationship.
How this can reduce frustration
Patients often feel dismissed when symptoms are intermittent. Clinicians often feel limited when they don't have enough rhythm data. Better documentation helps both sides.
A more productive conversation often starts with questions like these:
- “Do these tracings look consistent with AFib?”
- “Do you want more monitoring or imaging before calling this lone atrial fibrillation?”
- “Has my pattern changed enough to affect treatment?”
- “What would make you consider medication, blood thinners, or another test?”
Those are partnership questions. They are direct, respectful, and grounded in evidence.
When you combine your lived experience, your wearable data, and a clinician's judgment, the diagnosis becomes less mysterious. That usually lowers anxiety, even when the rhythm itself still needs attention.
Wondering if it's Atrial Fibrillation? On the Qaly app, human experts will interpret your ECGs for Atrial Fibrillation within minutes. Get started today.



.png)
.png)