

Key Takeaways

User Profile
Hello Heart Hero. If you are reading this, you may be tired of feeling your heart race, tired of trying medications that did not help enough, or tired of hearing about options that sound promising but still leave you with questions.
Many people reach this point after a long stretch of atrial fibrillation. They may have tried pills that slowed them down too much, or an ablation aimed at the atria that did not bring lasting relief. After a while, the goal often changes. Instead of chasing a perfect rhythm, you may want a heart rate you can live with and a day that does not revolve around symptoms.
That is where av node ablation enters the conversation. It is not the same as the afib ablation you may already know about. It is a different strategy, with a different trade-off, and for the right person it can offer a steadier, more predictable life.
If you want a broader look at common treatment for Afib, that can help place this option in context. For now, let’s focus on what makes this procedure unique and what it means for your daily life.
A New Path for Managing Your Heart Rhythm
A lot of patients come to this option feeling discouraged.
One person may say, “My watch keeps showing afib, my pulse jumps all over the place, and I cannot walk across the room without feeling drained.” Another may say, “I do not care if my rhythm is perfect anymore. I just want to stop feeling miserable.”
Those are very human reactions.
Av node ablation is often less about curing afib and more about taking back control from its symptoms. That distinction matters. It helps explain why some people feel relieved when they finally hear about it, while others feel nervous because it sounds so final.
Why this option can feel both hopeful and scary
The hopeful part is simple. If your main problem is a fast, irregular signal reaching the lower chambers of your heart, doctors can block that pathway.
The scary part is equally true. Once that pathway is intentionally blocked, you need a pacemaker to keep the ventricles beating in a steady way. That means this procedure is not a casual next step. It is a major decision.
Key takeaway: Av node ablation is a control strategy. It does not erase afib from the atria, but it can stop the chaotic atrial signals from controlling your pulse.
Why some patients prefer clarity over endless trial and error
People who feel skeptical about the healthcare system often have good reasons. They may have spent years bouncing between medication changes, emergency visits, and follow-ups that still did not answer their biggest question. “How do I live like this?”
Av node ablation can feel different because the goal is so concrete. It is not trying to persuade your heart to behave. It is creating a new electrical setup that is easier to manage.
For some families, that clear trade-off feels easier to understand than another round of “let’s see if this medicine works.”
What Is AV Node Ablation and Why Is It Different
Av node ablation treats a different problem than standard afib ablation.
A typical afib ablation targets areas in the atria that trigger or maintain atrial fibrillation. The goal is rhythm control. Doctors try to reduce or stop the abnormal rhythm itself.
Av node ablation does something else. It targets the atrioventricular node, which is the electrical bridge between the upper chambers and lower chambers. The goal is rate control. It blocks the chaotic atrial signals from reaching the ventricles.
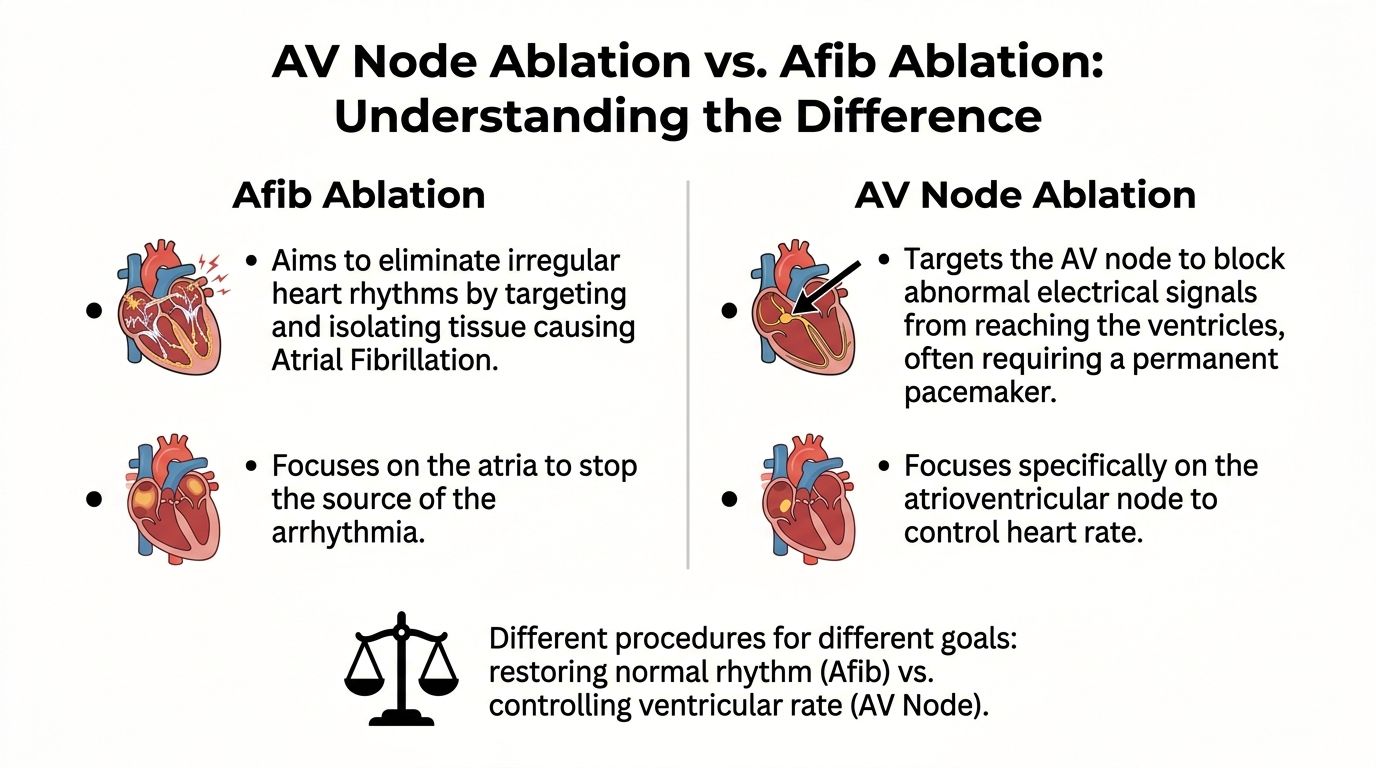
If afib is like a room full of people shouting, standard afib ablation tries to quiet the room. Av node ablation closes the soundproof door. The noise may still continue inside, but it no longer floods the rest of the house.
What the procedure changes
After av node ablation, the atria can still fibrillate.
What changes is that those fast, disorganized signals no longer drive the ventricles. Your pulse becomes controlled by a pacemaker instead of by the chaotic traffic coming from above.
That is why this procedure can bring major symptom relief even though it does not cure afib in the upper chambers.
If you are trying to understand how heart rhythm procedures fit together, a basic guide to cardiac electrophysiology can make the bigger picture easier to follow.
Why a pacemaker is not optional here
This is the point that often causes the most confusion.
The AV node is your heart’s normal electrical relay station. Once doctors intentionally destroy that relay, the ventricles need another reliable source of timing. That source is the pacemaker.
So the trade-off is direct:
- You lose the natural pathway: The normal electrical signal from atria to ventricles is interrupted on purpose.
- You gain a controlled pulse: The pacemaker takes over the job of setting the ventricular rate.
- You become pacemaker-dependent: This is a lifelong part of the plan, not a temporary bridge.
A detail that matters anatomically
A more precise, anatomical form of av node ablation targets the node just below the insulated His bundle. This can preserve a narrow QRS escape rhythm of 40 to 60 bpm, which is considered more physiologic than creating damage higher near the His bundle, where a wider and less stable escape rhythm can result, as described in this review of anatomical ablation at the atrioventricular node.
That sounds technical, but the practical message is simple. Where the lesion is placed can affect the quality of the backup rhythm.
Some readers also mix up rhythm emergencies and rhythm procedures. If that is you, this explanation of the difference between cardioversion and defibrillation may help sort out terms that often get blended together during stressful heart care discussions.
Who Is a Good Candidate for This Procedure
You might hear about AV node ablation after months, or even years, of trying to keep afib under control. The usual story is familiar. Your heart rate still jumps around, medications bring side effects, and daily life starts shrinking around symptoms. At that point, the question often changes from, "Can we stop afib completely?" to, "How do we stop afib from running the show?"
That is the group this procedure is often meant for.
AV node ablation is usually considered after other treatments have not given enough relief. The goal is not to cure afib in the atria. The goal is to protect the ventricles from fast, chaotic signals so your pulse becomes steady and predictable with a pacemaker. For many people, that trade-off can mean more energy, fewer frightening episodes, and more confidence leaving the house.
Patterns that often point toward this option
This path may be a fit if you experience several of the following:
- Medications have not slowed the heart rate enough: Your pulse still runs too fast, especially during afib episodes, or keeps changing in a way that leaves you feeling unwell.
- Rate-control drugs cause side effects that limit your life: You may feel tired, lightheaded, foggy, or too weak to do normal activities.
- Other treatments have already been tried: This can include medication changes, cardioversion, or a prior catheter ablation aimed at the atria.
- Symptoms remain a major problem: Shortness of breath, fatigue, dizziness, palpitations, and poor exercise tolerance often matter more than what the ECG looks like on paper.
- The practical goal is stable rate control, not a perfect rhythm: This is common in persistent or permanent afib, especially when rhythm-control strategies have not held up over time.
A simple way to frame it is this. Good candidates are often people whose afib symptoms keep disrupting ordinary life, even after careful treatment.
Why doctors call it "pace and ablate"
You may hear your cardiology team use the phrase pace and ablate. That means placing a pacemaker, then blocking the AV node so the lower chambers no longer race in response to the atria's chaotic signals.
This approach can make sense for someone who needs dependable rate control more than another round of rhythm chasing. It is often chosen for people with more complex health histories, where the desired outcome is better symptom control, fewer rate-related crashes, and a steadier day-to-day baseline.
If your doctor brings up this option, ask what problem they are trying to solve. Is it repeated ER visits? Ongoing exhaustion? A heart rate that still spikes despite medication? That question helps families understand why this procedure is different from treatments that aim to restore normal rhythm.
You may also hear that the procedure is done with imaging guidance, often using X-ray. If that term is unfamiliar, this plain-language guide on what fluoroscopy is during heart procedures can make the process easier to follow.
Clinical perspective: The best candidate is usually the person whose symptoms, medication tolerance, and treatment history point toward pacemaker-based rate control as the clearest path to a more livable routine.
When quality of life becomes the main goal
For some older adults, and for some people with several heart or medical conditions, the target shifts. The target becomes a steadier pulse, fewer symptoms, and more predictable days.
That is not settling.
It is a thoughtful decision about control. AV node ablation does not erase afib, but it can stop afib from dictating how you feel hour by hour. For many patients, that is the moment this option starts to make sense.
Your AV Node Ablation Journey Step by Step
Many patients feel less anxious when they know what the day will look like.
In many cases, the pacemaker is implanted first, either in the same session or shortly before the ablation. That is done because once the AV node is ablated, you need dependable pacing right away.
Before the procedure
You will usually arrive having followed instructions about food, drink, and medications.
The team checks your vitals, reviews your history, and confirms the plan. If you are having both pacemaker placement and ablation, the conversation often centers on safety, comfort, and the order of the steps.
A lot of people worry they will be fully awake and frightened. In reality, the team uses sedation or anesthesia based on your situation, your health, and the exact approach being used.
During the pacemaker part
The pacemaker is placed to make sure your ventricles have a reliable rhythm source.
Doctors insert leads and secure the device so that when the AV node is later blocked, your heart still has a steady beat. In some settings, a superior approach through the axillary vein is used, especially when a device procedure and AV node ablation are being combined.
During the ablation itself
The doctor threads a catheter to the area of the AV node and applies energy to interrupt conduction.
In a superior approach used with device implantation, the mean radiofrequency delivery time to create complete heart block was 110 ± 43 seconds, the total procedure averaged 87 ± 21 minutes, and anatomical localization was 100% in the report describing this technique via the superior vena cava approach for AV node ablation.
Those numbers often surprise people. The setup and careful positioning take time, but the delivery of energy can be brief.
If you are unsure what X-ray guidance looks like during heart procedures, this plain-language explanation of what a fluoroscopy is can help.
What you may feel
Experiences differ, but many patients remember pressure, positioning, and the odd feeling of being in a monitored procedure room more than they remember pain.
Some feel sleepy. Some remember very little. The team watches your rhythm, blood pressure, and pacing function the whole time.
Right after the procedure
Recovery usually starts with monitoring, rest, and device checks.
A nurse watches the access site, helps manage discomfort, and makes sure the pacemaker is working as expected. If both procedures were done together, you may also get instructions about arm movement and incision care.
A simple way to think about the immediate recovery period is this:
- The pacemaker takes over the job of setting ventricular rate
- The team confirms the AV node block is complete
- You begin learning life with your new pacing system
Practical tip: Ask before discharge who to call for wound concerns, what symptoms should prompt urgent evaluation, and when your first pacemaker check will happen.
Weighing the Benefits and Significant Risks
This choice deserves honesty.
The main benefit of av node ablation is not subtle. For the right patient, it can replace a wildly unpredictable pulse with a stable ventricular rate. That can mean less pounding, less breathlessness, less exhaustion, and fewer days built around symptom avoidance.
What many patients gain
The procedure is regarded as highly effective at accomplishing its technical goal.
A Northern Irish registry reported successful ablation in all patients, with a median procedure time of 55.5 minutes, median fluoroscopy time of 3.5 minutes, median radiation dose of 11 mGy, and zero acute or subacute complications up to three months. The same review notes a 0.87% adverse event rate in a Swedish registry and says Cleveland Clinic reports a success rate nearly 100% in this summary of real-world AV nodal ablation registry data.
That does not mean every patient feels perfect afterward. It means the procedure is very good at achieving complete AV block and steady rate control.
The trade-off that matters most
The biggest issue is not a rare complication. It is the intended result.
You become dependent on a pacemaker for ventricular rhythm. For many people, that is a worthwhile exchange. For others, it feels emotionally heavy.
Common concerns include:
- Device dependence: You rely on the pacemaker every day.
- Future device care: You will need follow-up checks and eventual generator changes.
- Adjustment period: Some people need time to trust the device and their “new” pulse.
- Ongoing afib above the ventricles: The atria can still fibrillate even when the pulse feels steady.



The usual procedure risks
Even safe procedures still carry ordinary medical risks.
These can include bleeding, bruising, infection, discomfort at the insertion or device site, and the usual risks that come with catheter work and implanted hardware. Your own risk profile also depends on age, kidney function, frailty, and the reason this strategy is being chosen in the first place.
Balanced view: Av node ablation is often technically successful and procedurally safe. The most important decision is whether symptom control is worth permanent pacemaker dependence for you.
Looking beyond the procedure day
When families hear “safe and effective,” they sometimes think that settles everything. It does not.
What matters just as much is whether this strategy fits your goals, your other health conditions, and your willingness to live with a pacing device long term. Nuance matters here. That is where the most important conversations happen.
Life After Ablation Your New Normal with a Pacemaker
The first surprise for many people after av node ablation is that a steady pulse does not mean afib disappeared.
Your pacemaker may keep the ventricles regular, but the atria can still be in fibrillation. If you only check your pulse with your fingers, you may think the rhythm problem is “gone” when what really changed is that the lower chambers are now protected from the chaos above.
What daily life often looks like
Many people settle into routines that feel ordinary again.
You may have device checks, some restrictions during healing, and new awareness of your pacing system. Then life gradually becomes less about reacting to sudden heart rate swings and more about noticing patterns, symptoms, and energy level.
Daily life after healing often includes:
- Pacemaker follow-up: Regular checks make sure the device settings still fit your needs.
- Symptom tracking: Even with good rate control, fatigue, palpitations, or shortness of breath still deserve attention.
- Medication review: Some medicines stay, some change. Your clinician guides that part.
- Rebuilding confidence: Walking, errands, travel, and exercise often feel less intimidating when your pulse is no longer racing unpredictably.
Why rhythm monitoring still matters
A major education gap is that av node ablation does not stop the atria from fibrillating, and that ongoing atrial activity can go unnoticed when the pulse is controlled by a pacemaker. This gap, along with the potential value of wearable ECGs for tracking what is still happening electrically, is discussed in this patient-centered article on why you should not have AV node ablation.
That article argues from a skeptical angle, but it highlights something useful. A controlled pulse can hide the fact that afib continues in the atria.
For patients with Apple Watch, Kardia, Fitbit, Samsung, or similar devices, this matters because wearable ECGs can help you notice trends, document episodes, and bring more useful information to your medical appointments.
Emotional recovery counts too
Some people feel immediate relief. Others feel uneasy at first.
It is common to ask:
- Is the pacemaker doing enough?
- Why do I still feel odd beats sometimes?
- If my watch still shows afib, did the procedure fail?
Those questions do not mean something went wrong. They often mean nobody fully explained the difference between symptom control and rhythm elimination.
If you or your family needs more hands-on recovery help at home, practical resources about in-depth nursing support can also make the transition less stressful, especially after a hospitalization or new device placement.
If you want a plain-language overview of what it means to live with a pacing device, this guide to heart pacemaker operation can help.
Most important mindset shift: After av node ablation, your goal is not to “feel the afib disappear.” Your goal is to live better with a protected, paced ventricular rhythm.
Frequently Asked Questions About AV Node Ablation
Does the pacemaker stop my afib
The pacemaker does not stop atrial fibrillation. Its job is to keep the lower chambers beating at a steady, reliable rate after the AV node is ablated.
That difference matters. AV node ablation is usually about symptom control and rate control, not removing afib from the atria. For many patients, the win is a calmer, more predictable pulse that lets daily life feel manageable again.
If my watch still shows afib, does that mean the procedure failed
A watch reading can still show afib after the procedure, and that can be upsetting if no one warned you.
The procedure can still be doing exactly what it was meant to do. The atria may continue to fibrillate, but those chaotic signals are no longer driving the ventricles. Your pacemaker takes over that job and keeps the heart rate from swinging wildly.
So success is measured by control, not by making every wearable tracing look normal.
Will I feel the pacemaker working
Usually, no.
You may not feel each paced beat at all. What many patients notice instead is that the old pounding, racing, or uneven feeling settles down. Early on, some people are very aware of the device because it is new and they are paying close attention to every sensation. That usually eases with time.
Can I still exercise and travel
Many patients return to walking, errands, travel, and other usual activities after healing and medical clearance.
The safer question is not whether you can be active. It is how much activity fits your whole heart picture, including heart failure, valve disease, lung disease, and your pacemaker settings. Your care team can help you find the line between healthy activity and overexertion.
What should I make of long-term outcomes
This question deserves a careful answer.
People who have AV node ablation are often older or already dealing with significant heart disease. That makes long-term outcome numbers hard to interpret at a glance. A poor outcome years later does not automatically mean the procedure caused it. In earlier research, investigators noted that patients selected for this strategy often carried a heavier illness burden from the start, which is why results must be read in context, as noted earlier.
The practical takeaway is simpler. AV node ablation is usually chosen when symptoms, fast rates, or medication side effects are taking too much away from daily life. The trade-off is clear. You become dependent on a pacemaker, but in return you may gain a steadier heart rate and more control over how you feel day to day.
Get clarity on your ECG readings. Upload your wearable data to Qaly and understand your heart rhythm before your next cardiology visit.



.png)
.png)