


Key Takeaways

User Profile
Hello Heart Hero. You feel a strange flutter in your chest, then your mind starts racing. Was that anxiety, too much caffeine, poor sleep, or could your birth control be involved?
That question makes sense. When your heart feels different, even for a few seconds, it can be hard to think about anything else. A lot of people also worry they’ll be brushed off if they bring up symptoms that come and go, especially when those symptoms don’t happen right in front of a doctor.
If you’re trying to figure out whether hormones could be playing a role, you’re not overreacting. You’re paying attention to your body. And if you want a better sense of what people mean by “palpitations,” this guide on what heart palpitations feel like can help you put words to the sensation.
That Fluttering Feeling and The Questions It Brings
A common story goes like this. Someone starts a new pill, patch, or ring. A few days or weeks later, they notice a skipped beat while folding laundry, climbing stairs, or lying in bed at night. Nothing dramatic happens, but now they’re hyper-aware of every sensation in their chest.
That doesn’t mean the symptom is “all in your head.” It means your body gave you a signal, and you’re trying to understand it.
Palpitations can feel different from person to person. For one person, it’s a flutter. For another, it’s a pounding heartbeat, a pause, or a sudden thump. The feeling can be brief and harmless, but it can still be unsettling because the heart is one of those body systems we’re wired to take seriously.
Your concern is valid even if the symptom is brief, intermittent, or hard to prove.
People often get stuck between two fears. One is, “I’m ignoring something important.” The other is, “I’m going to be told this is stress and sent home.” Both worries are understandable.
Why this question comes up so often
Birth control changes hormone levels. Hormones influence many body systems, including the cardiovascular system. So when a new symptom shows up after starting, stopping, or switching contraception, it’s natural to connect the dots.
Sometimes that connection is real. Sometimes the timing is coincidental. Often, it takes careful tracking to tell the difference.
What helps right away
Before you assume the worst, try to get specific about the experience:
- Notice the sensation: Was it a flutter, a hard pound, a racing spell, or a skipped beat?
- Watch the timing: Did it begin after starting a new method or changing doses?
- Look for patterns: Does it happen at rest, after caffeine, during stress, or around the same time of day?
- Check for other symptoms: Chest pain, fainting, severe shortness of breath, or feeling like you might pass out need prompt medical attention.
You don’t need to solve everything tonight. But you can start gathering clues.
The Short Answer on Birth Control and Palpitations
Yes. Can birth control cause heart palpitations? For some people, yes.
The reassuring part is that this answer is more nuanced than it sounds. A palpitation after starting birth control does not automatically mean something dangerous is happening. It does mean hormonal contraceptives can change body chemistry enough to trigger or worsen palpitations in some people, especially people who are already sensitive to hormone shifts or who have other heart-related risk factors.
A practical way to picture it helps. Your heart rhythm usually keeps steady time, like a piano that stays in tune. Hormone changes can act like a shift in temperature in the room. Sometimes nothing sounds different. Sometimes one key starts to sound a little off, and you notice a flutter, skip, or hard thump that was not there before.
Birth control also is not one single exposure. Some methods use estrogen and progestin together. Others use progestin only. Some mainly work locally, such as hormonal IUDs, while others send more hormone through the bloodstream, such as pills, patches, or rings. That helps explain why one person feels no change at all and another notices symptoms soon after starting, stopping, or switching methods.
Your response can depend on several things:
- The specific hormones in the method
- How sensitive your body is to hormone changes
- Your age, smoking status, and medical history
- Whether you already have a tendency toward palpitations, arrhythmias, or clotting problems
- Whether another issue is happening at the same time, such as stress, dehydration, caffeine use, or symptoms linked with low estrogen and hormone imbalance
Bottom line: Birth control can be part of the picture, but it is rarely the whole story.
That is why the most useful question is usually not, “Is birth control always the cause?” A better question is, “Could this method be affecting my body, and how can I document what is happening?”
For many people, that shift lowers anxiety. You move from guessing to observing. If you are worried your symptoms will be brushed off, tracking episodes with timestamps, symptom notes, heart rate data, or a wearable ECG can give you something concrete to bring to a doctor. Tools like Qaly can also help review rhythm recordings so you are not relying on memory alone when you ask for care.
How Hormones Can Affect Your Heart's Rhythm
Your heart doesn’t beat by accident. It runs on a built-in electrical system that tells each beat when to start, squeeze, and reset. When that electrical timing changes, even slightly, you may feel a flutter, skip, or racing spell.
Hormones can influence that timing. That’s the key reason birth control can sometimes play a role in palpitations.
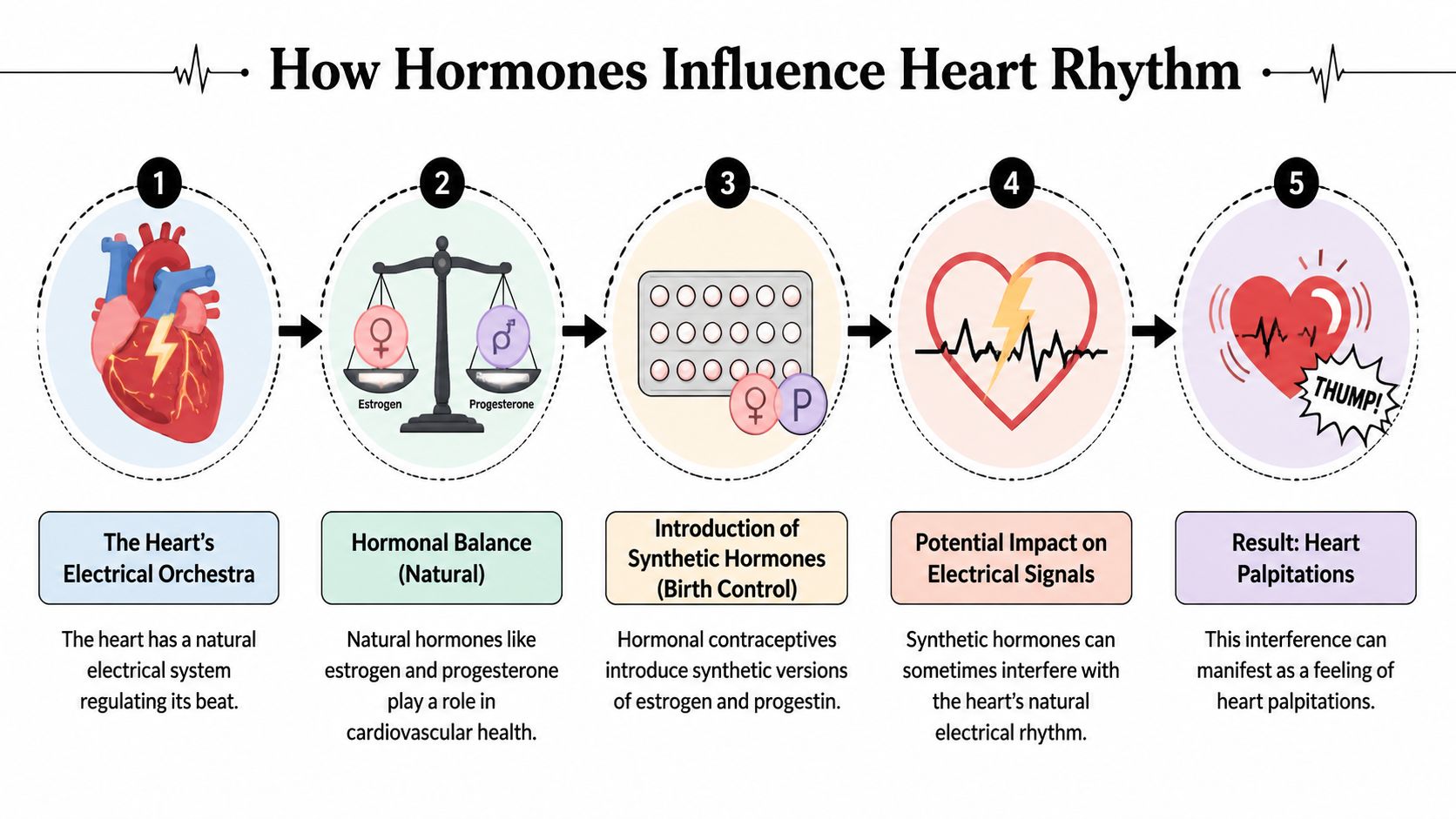
The orchestra analogy
A helpful way to picture this is to think of your heart as an orchestra. The electrical system is the conductor. Each heart cell is an instrument waiting for its cue.
Hormones like estrogen and progesterone can influence how those instruments respond. If the timing shifts, the music can still continue, but you may notice a beat that feels too early, too forceful, or slightly out of rhythm.
According to this explanation of hormonal changes and heart palpitations, hormonal birth control can affect cardiac electrophysiology directly. Estrogen influences the delayed rectifier potassium current, or IKr, which can prolong the QT interval, a known trigger for arrhythmias. Progesterone can have a counter-effect, but combined oral contraceptives may still lean toward estrogen’s influence, which can increase sinus node automaticity and sympathetic tone.
What that means in plain language
You don’t need to memorize terms like IKr or QT interval. Here’s the simpler version:
- Your heart has electrical recharge time: After each beat, it resets for the next one.
- Estrogen can affect that reset process: In some people, it may make the electrical system more likely to misfire.
- Progesterone doesn’t always cancel that effect out: The hormone mix matters.
- A more “excitable” electrical system can create palpitations: You feel the result as a flutter, skip, or racing beat.
If you’ve ever noticed that symptoms show up with hormonal changes in other parts of life, this broader discussion of symptoms of low estrogen may also help you see how strongly hormones can affect the body beyond reproduction alone.

Why some people feel every little change
Two people can have the same extra beat, and only one notices it. That’s part biology, part nervous system sensitivity.
If your heart throws in an occasional early beat, you may feel:
- A pause
- A flip-flop sensation
- A sudden hard thump
- A quick burst of fluttering
Those sensations can feel intense even when the rhythm change is brief.
A benign rhythm hiccup can feel dramatic. Sensation and danger are not the same thing.
That’s one reason people get confused. The feeling can be scary, while the underlying issue may be mild. Still, if the symptom is new after starting birth control, it deserves attention rather than dismissal.
Comparing Different Birth Control Types and Their Risks
Different birth control methods can affect the heart in different ways. That matters because a fluttery feeling after starting a new method can leave you asking, “Is this a coincidence, or is my body reacting to something real?”
A helpful way to sort this out is to group methods by what hormones they use and how much of those hormones circulate through the body. The method itself is only one piece of the puzzle, but it gives you a practical place to start.
Combined hormonal methods
This group includes combined oral contraceptive pills, the patch, and the ring. They all contain estrogen plus a form of progestin.
These methods get the most attention in conversations about palpitations because estrogen is the hormone more often linked to changes in heart rhythm, blood pressure, and clotting risk in some people. That does not mean every combined method is dangerous, or that every flutter means harm. It means this category deserves a closer look if symptoms started after you began using it.
Research has also been mixed rather than one-directional. In a large cohort, overall oral contraceptive use was linked with a lower overall rate of cardiovascular events, while a separate trial found that women with long QT syndrome who used progestin-only oral contraceptives without beta-blockers had a higher risk of cardiac events. Both findings were summarized in a single Heart Rhythm Society report on contraceptive use and cardiac risk. The big takeaway is simple. Population-level averages do not erase the fact that some rhythm conditions need very individualized decisions.
Progestin-only methods
This category includes the mini-pill and other progestin-only options.
People often hear “progestin-only” and assume it automatically means lower heart risk. Real life is more specific than that. For many people, these methods may be a reasonable option, especially if estrogen is a concern. For a person with a known rhythm disorder, though, the safer choice depends on their diagnosis, their other medications, and the exact symptom pattern they notice.
That distinction matters because “better for some people” is not the same as “best for everyone.”
IUDs, injections, and implants
These options can feel harder to compare because they differ in dose, delivery, and how much hormone reaches the whole body. A hormonal IUD often has lower systemic hormone exposure than the pill, while injections and implants can create a different hormone pattern over time.
Here is a practical way to look at them:
- Hormonal IUDs: Often chosen by people who want less whole-body hormone exposure, though some still notice new palpitations or other symptoms.
- Injectable or implantable methods: These work well for many people, but timing still matters. If symptoms begin soon after starting one, that pattern is worth tracking.
- Patch users: The patch belongs in the combined hormonal group, so it helps to review common contraceptive patch side effects if you are trying to connect symptoms with timing.
If you do notice fluttering, skipped beats, or a racing sensation after switching methods, try to treat that observation like a clue, not a verdict. Write down when the symptom happens, what method you are using, when you started it, and whether caffeine, stress, poor sleep, or exercise seem to play a role. If you do not fully trust that a rushed appointment will capture the pattern, tools like a wearable ECG or Qaly can help you collect rhythm data you can bring to your doctor. That can turn a vague “something felt off” into a clearer conversation.
The bigger decision is rarely just about palpitations
Birth control choices often involve several concerns at once. Some people are weighing symptom control, pregnancy prevention, migraine history, blood pressure, acne, mood changes, or family history all at the same time.
If you’re trying to understand hormonal tradeoffs more broadly, this resource on connections between hormones and cancer offers useful context about another concern people often discuss alongside birth control decisions.
The clearest conclusion is this: the right method depends on your body, your medical history, and what your symptoms are doing over time. Good tracking can make that decision less confusing and much more grounded in evidence from your own life.
Understanding Your Personal Risk Factors
The birth control itself is only part of the story. Your health history changes the picture.
Who may need more caution
According to Hartford HealthCare cardiology guidance summarized here, estrogen in combination birth control boosts liver production of clotting factors, which raises thrombosis risk. The same source notes that the risk is generally small, but it needs more careful consideration in smokers, women over 35, and people with a family history of coronary disease.
That matters because clotting, blood pressure changes, and strain on the cardiovascular system can all overlap with symptoms people describe as pounding, racing, or palpitations.



A simple self-check
Ask yourself these questions:
- Do you smoke? Smoking adds cardiovascular strain and can change the risk calculation.
- Are you over 35? Age can shift how carefully estrogen-containing methods should be weighed.
- Do you have a family history of heart disease or rhythm problems? Family patterns matter.
- Have you ever been told you have high blood pressure, diabetes, or a prior stroke history? These conditions can change which options make sense.
- Do you already know you have a rhythm condition? If so, your contraceptive choice deserves a more individualized discussion.
If you want a broader framework for thinking about your baseline heart risk, this guide to a risk score for cardiovascular disease can help you understand the kinds of factors clinicians often consider.
Why personal context matters more than internet averages
A healthy nonsmoker in her twenties with no cardiac history is not starting from the same place as someone who smokes, has hypertension, and has relatives with early heart disease. The same prescription can carry a very different practical meaning depending on the person.
Reality check: “Common” and “safe for many” are not the same as “right for me.”
Skepticism of the healthcare system can be productive. You don’t have to accept vague reassurance, and you also don’t have to assume the worst. You can ask for a discussion that looks at your full picture, not just a generic handout.
How to Monitor Palpitations and Talk To Your Doctor
You feel a sudden flutter, your stomach drops, and by the time you consider getting help, it is gone. That is one reason palpitations can feel so upsetting. The symptom is real, but it can be hard to prove in the moment.
A good next step is to turn a vague, stressful experience into a clear record. That gives you something more useful than memory alone, especially if you have felt brushed off before.
Turn a symptom into a record
Use a note on your phone, a paper journal, or whichever method you can keep up with. The goal is not perfection. The goal is pattern recognition.
Write down:
- When it happened
- What it felt like
- What you were doing right before it
- Whether caffeine, alcohol, stress, poor sleep, dehydration, or exercise were involved
- Where you were in your pill pack or hormone cycle
That last detail can be surprisingly helpful. If episodes show up after starting a new method, during active pills, or around a switch, your clinician has a better starting point for figuring out whether hormones may be part of the story.
Use tools that capture the moment
Palpitations are a bit like a skipped scene in a movie. You know something happened, but a recording helps other people see it too.
If you have an Apple Watch, Kardia, Fitbit, Samsung watch, or another wearable ECG device, try to record a tracing during symptoms. Even a single captured episode can make the discussion much more concrete.
Qaly is one practical option for reviewing wearable or at-home ECGs. Users can upload recordings for review by certified cardiographic technicians, and the reports may include rhythm interpretation and interval measurements such as PR, QRS, and QTc. If your symptoms seem tied to a medication change, that kind of documentation can help you bring clearer information to your doctor.
No device? Your log still matters. A careful symptom history often gives important clues even without a tracing.
Bring your doctor organized information
You do not need a color-coded spreadsheet. A simple folder, screenshot album, or phone note is enough.
Bring:
- A symptom timeline
- The name of your birth control method
- The date you started, stopped, or switched it
- Any captured ECGs
- A short list of patterns or triggers you’ve noticed
This can shift the conversation in a useful way. Instead of saying, “I get random flutters,” you can say, “These started after I changed methods, here are the dates, and here is what I recorded when it happened.”
Good data does not replace medical care. It helps your symptoms speak more clearly.
Don’t ignore the anxiety loop
Palpitations can trigger fear fast. Fear can then make your heart race harder, which makes the whole episode feel even more alarming. That loop is common, and it does not mean you are imagining anything.
What to ask at the appointment
You do not need to sound like a cardiologist. Clear, direct questions are enough:
- “Could this birth control method be contributing to my palpitations?”
- “Based on my history, is estrogen a concern for me?”
- “Do these episodes mean I should have an ECG or see cardiology?”
- “Would a different contraceptive option make more sense?”
- “If this happens again, what signs mean I should seek urgent care?”
If you have ever felt dismissed, bringing a timeline and recordings can help keep the visit grounded in specifics. You are not asking for too much. You are giving your doctor the pieces they need to make a better decision with you.
Your Next Steps Toward Heart Health and Peace of Mind
If you’ve made it this far, you already have the most important starting point. You’re paying attention.
Yes, birth control can be related to palpitations in some people. But that doesn’t mean you’re in danger, and it doesn’t mean you have to choose between suffering in silence and quitting your contraception overnight. It means there may be a real, understandable connection worth checking carefully.
A calm plan works better than a panicked one
Start with observation. Track when the palpitations happen, how long they last, and what else was going on. Notice whether the episodes cluster around a change in contraception, stress, sleep disruption, caffeine, or dehydration.
Then gather evidence when you can. If you have a wearable ECG device, use it during symptoms. If you don’t, the symptom log still matters. Patterns are often more revealing than a single scary moment.
Give yourself permission to ask better questions
You are allowed to say:
- “This symptom started after I changed birth control.”
- “I want to understand whether estrogen is a good fit for me.”
- “I’d like a plan if this keeps happening.”
Those are reasonable requests. They’re not dramatic. They’re part of informed care.
Remember what the goal is
The goal is not to prove yourself right. The goal is to understand what your body is doing and make a safer, more comfortable decision from there.
Sometimes that decision is staying on the same method with reassurance. Sometimes it’s switching to another option. Sometimes it’s finding out the palpitations have more to do with stress, sleep, or another health issue than with contraception itself.
What matters is that you don’t have to stay stuck in uncertainty. You can move from fear to information, and from information to action.
Capture palpitations as they happen. Qaly turns wearable ECG recordings into reviewed reports you can share with your clinician.



.png)
.png)