


Key Takeaways

User Profile
The procedure is over. You wanted relief, a steadier rhythm, maybe a little less fear. Then a few days or weeks later, your chest does something odd. A flutter. A skip. A burst of fast beats that feels uncomfortably familiar.
That moment can shake you. Many people immediately think, “It didn't work.”
That reaction makes sense. Atrial fibrillation after ablation is one of the most confusing parts of recovery because the timeline is not intuitive. Some rhythm changes are expected. Some deserve a closer look. And the gap between those two ideas is where anxiety tends to grow, especially if you're staring at a wearable ECG and trying to make sense of a result on your own.
This guide is here to make that period less murky. I'm going to walk you through what can be normal, what might signal recurrence, how doctors confirm what's happening, and how your own wearable ECG can help you respond calmly instead of rushing into panic.
Your Post Ablation Journey Begins
Hello Heart Hero. You may be reading this with your phone in one hand and your pulse under your fingers, wondering whether the sensation you just felt is harmless healing or the return of AFib.
A lot of people imagine ablation as a clean before-and-after moment. Procedure done, rhythm fixed, life back to normal. Real recovery is usually messier than that. Your heart has been treated, but it still needs time to settle. During that time, sensations can be noisy, inconsistent, and emotionally exhausting.
One patient told me the hardest part wasn't the procedure itself. It was the days after, when every skipped beat felt like a verdict. She kept asking herself whether she was overreacting or missing something serious. That tug-of-war is common.
You are not failing recovery because you notice symptoms. You are paying attention to your body during a vulnerable moment.
What helps most is replacing vague fear with a working map. If you know the usual rhythm of healing, you can stop treating every flutter like an emergency. You can also communicate more clearly with your electrophysiologist or cardiology team.
If you want another patient-friendly overview of the recovery phase, this life after cardiac ablation guide can help you frame what day-to-day recovery may look like.
For now, hold onto this: feeling something after ablation does not automatically mean the ablation failed. The timing, pattern, and ECG details matter.
The Blanking Period Understanding the First Three Months
The first three months after ablation are often called the blanking period. That term matters because it explains why early rhythm episodes aren't judged the same way as episodes that happen later.
Your heart tissue has just been treated. It can be irritated and inflamed while the lesions heal and mature. A scraped knee is a good comparison: It may look red and angry before it settles down. That doesn't mean the skin won't heal. It means healing is active.

Why symptoms can happen early
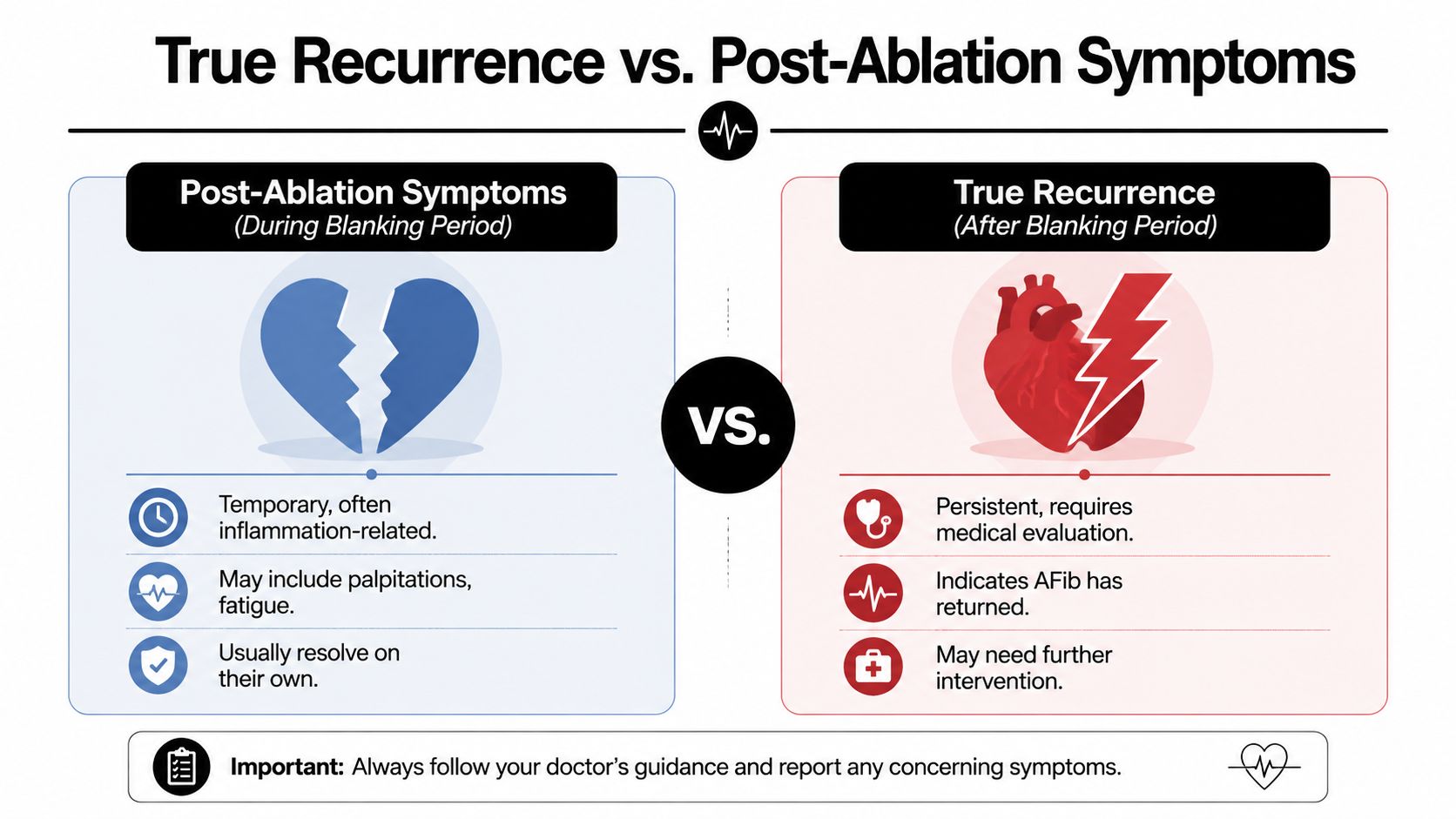
During this window, people may notice palpitations, brief runs of rapid rhythm, extra beats, or short bursts that feel a lot like the arrhythmia they had before. That overlap is exactly why this period creates so much confusion.
A Cleveland Clinic discussion on post-ablation AFib notes that the first 3 months are treated as a blanking period because early episodes often reflect inflammation and lesion maturation rather than definitive failure. It also notes that early recurrence of AF or atrial flutter within this window occurs in approximately 50% of patients in some series, and repeat ablation is generally deferred for at least 3 months when possible, according to this Cleveland Clinic podcast episode on AFib after ablation.
That statistic surprises many patients. It shouldn't scare you. It should normalize what can otherwise feel alarming.
What to do during the blanking period
Your job during these weeks is observation, not instant conclusion.
A good approach looks like this:
- Capture the moment: If you have an Apple Watch, Kardia, Fitbit, Samsung watch, or another single-lead ECG device, record an ECG when symptoms happen.
- Label the recording: Note what you felt. Fluttering, pounding, skipped beats, dizziness, chest discomfort, or shortness of breath.
- Track the pattern: Was it a brief burst, several minutes, or something that kept going?
- Avoid spiraling: Taking repeated ECGs every minute often raises anxiety without adding useful information.
Practical rule: A symptom during the blanking period is a data point, not a final answer.
What not to assume
Don't assume every post-ablation rhythm change is AFib. Some people have premature beats. Some have atrial tachycardia. Some have brief, self-limited irregularity that fades as healing continues. Wearables can help catch these moments, but the reading still has to be interpreted in context.
This is why the first three months can feel emotionally hard. You're healing, but the heart doesn't always sound quiet while it heals.
True Recurrence What AFib After the Blanking Period Means
Once you're beyond the blanking period, the conversation changes. Rhythm episodes after that window carry more weight because the healing-related noise should be easing off.
That doesn't mean every later symptom is definitely atrial fibrillation. It means the possibility of true recurrence becomes more relevant and deserves proper evaluation.
Temporary healing versus late return
The easiest way to separate these ideas is by cause.
Early post-ablation rhythm trouble is often related to healing tissue. Late recurrence is often related to pulmonary vein reconnection, which means areas that were electrically isolated can reconnect over time and allow AFib triggers to return.
That can be frustrating to hear. It can also be oddly reassuring. If AFib comes back, it doesn't automatically mean your body “rejected” the procedure or that the first ablation was pointless. It often reflects how complex AFib is.
What long-term expectations really look like
A patient advocacy summary of AF ablation outcomes notes that single-procedure success rates are approximately 60% or higher for paroxysmal AF and 30% or less for persistent AF. After multiple procedures, success rates improve to 70% or higher for paroxysmal AF and 50% or higher for persistent AF. The same summary notes that very long-term follow-up beyond 3 years shows recurrence after a single procedure in roughly 52% of paroxysmal and 61% of persistent AF patients, while multiple procedures reduce recurrence to 19% and 29% respectively. It also notes that AF often recurs in 40% to 50% of cases beyond the first year, as outlined in this StopAfib review of catheter ablation success rates.
Those numbers are worth reading slowly. Ablation helps many people. It also isn't always a one-time cure.
A recurrence after ablation is disappointing, but it is not unusual, and it is not the end of your treatment options.
What patients often get wrong
People often think recurrence means they are back at square one. Usually that isn't how clinicians see it. Your symptom burden may still be lower. Episodes may be shorter. Medicines may work better than they did before. And if a repeat procedure is needed, the second strategy can be more targeted because your team has learned something from the first one.
Atrial fibrillation after ablation is better understood as an ongoing management path, not a pass-fail test.



How Doctors Confirm if Your AFib is Back
When symptoms return, doctors try to answer two separate questions. First, what rhythm is happening? Second, how often is it happening and how much is it affecting you?
That's why your cardiology team may use different monitoring tools instead of relying only on one office ECG.
The tools they commonly use
Some people get a short-term Holter monitor. Others get an event monitor they activate when symptoms happen. For people with less frequent episodes, a longer-term monitor may make more sense. Your doctor chooses based on your symptom pattern, not because one monitor is always better.
If you want a plain-language overview of how these monitors differ, this cardiac event monitor explainer is useful.
Here's the key issue. Many rhythm problems are intermittent. A normal clinic ECG doesn't rule out recurrence if your symptoms come and go.
Why your wearable ECG can matter
A single-lead tracing from your Apple Watch, Kardia, Fitbit, Samsung watch, or similar device can be very helpful if it captures the rhythm during symptoms. Sometimes that home tracing becomes the clearest evidence of what's happening because it records the exact moment you felt the problem.
Bring those ECGs to your appointment. Keep the recordings, the timestamps, and a short symptom note. That saves time and gives your clinician something more useful than “I felt weird last Tuesday.”
The most valuable ECG is often the one recorded during the symptom, not the one taken hours later when everything feels normal.
If a repeat procedure comes up
Many patients worry about safety if their doctor mentions another ablation. It helps to know that the procedure has become safer over time. A JACC analysis found that overall complication rates for catheter ablation of AF declined from 5.3% in 2013 to 2017 to 3.7% in 2018 to 2022, and severe complications declined from 3.1% to 1.9%, according to this JACC report on AF ablation complications and mortality.
That doesn't make the decision simple, but it does provide context. If recurrence is confirmed, your team isn't offering a repeat procedure casually. They're weighing symptoms, rhythm burden, stroke risk, medications, and your overall goals.
Your Role Using Wearable ECGs for Smart Monitoring
This is the part many patients are never really taught. A wearable ECG is most useful when you use it with a plan.
If you record constantly, you can overwhelm yourself with noise. If you never record during symptoms, you may miss the exact information your clinician needs. The sweet spot is focused, calm monitoring.

A simple way to use your device well
When you feel something, pause. Sit down if you can. Relax your shoulders and take a steady breath before recording. Then take one ECG.
After that:
- Save the strip: Don't rely on memory.
- Name the symptom: “Flutter,” “racing,” “skipped beats,” or “felt lightheaded” is enough.
- Write the context: Resting, walking, after coffee, after poor sleep, after a meal, or during stress.
- Watch for duration: Brief and self-limited feels different from persistent and escalating.
This helps because atrial fibrillation after ablation is not just about whether a rhythm happened. It's about pattern, timing, and how your symptoms line up with the tracing.
Why inconclusive results feel so stressful
Wearables are useful, but they can also be unnerving. You may get “inconclusive,” “poor recording,” or a rhythm label that doesn't match how you feel. That's common with consumer devices. A noisy strip can look alarming even when it doesn't show sustained AFib.
For some patients, that uncertainty is the worst part. They don't know whether to rest, call the office, or head to the emergency room.
One option is to use a human-reviewed ECG service rather than relying only on an automated label. For example, Qaly's continuous monitoring overview describes a service that reviews wearable and at-home ECG recordings with certified cardiographic technicians and reports rhythm interpretation plus interval details such as PR, QRS, and QTc. That kind of review can help distinguish a benign ectopic pattern from something that needs faster follow-up.
Here's a quick walkthrough of the idea in video form.
What smart monitoring is not
It is not checking your rhythm every few minutes because you're scared. It is not trying to diagnose yourself in isolation. It is not replacing your electrophysiologist.
It is using the tools you already own to create cleaner information, lower guesswork, and reduce unnecessary panic. When done well, wearable monitoring can help you decide whether you're seeing a minor blip, a pattern worth messaging your doctor about, or a true urgent problem.
What Happens If AFib Returns Treatment Options
If AFib is confirmed after the blanking period, the next step depends on your symptoms, how long the episode lasts, your other medical conditions, and whether you're already taking rhythm or rate medications.
Some people need only a medication adjustment. Others may be offered cardioversion to restore sinus rhythm. For some, a repeat ablation becomes the most reasonable path.
The usual decision path
Doctors often think through recurrence in layers:
- Medicines first: Sometimes the rhythm can be stabilized with antiarrhythmic or rate-control medication, especially if episodes are not constant.
- Cardioversion when needed: If you're stuck in AFib and it's causing symptoms, cardioversion may be used to reset the rhythm.
- Redo ablation for ongoing trouble: If episodes keep returning or symptoms remain disruptive, another ablation may be discussed.
Blood thinners are part of this conversation too. Many patients assume that if they've had an ablation, anticoagulation is automatically finished forever. That is not always the case. Stroke prevention decisions depend on your overall risk profile, not just whether you had a procedure in the past. Your clinician should guide that choice.
Why a second ablation is not a failure
This point matters emotionally. People often hear “repeat ablation” and think the first procedure was wasted. That's not how electrophysiology works.
A study on long-term outcomes after recurrent AF found that among patients whose recurrence was significant enough to undergo repeat procedures, success on second ablation was 57% at 5-year follow-up, and overall freedom from AF rose from 52% to 66% after the second procedure, according to this Circulation Arrhythmia and Electrophysiology study on repeat ablation outcomes.
Those numbers don't promise success for every individual. They do show that another procedure can be a standard, evidence-based next step rather than a last resort.
If you want a broader plain-language summary of how recurrence can be treated, this treatment for AFib guide is a helpful companion read.
Frequently Asked Questions About Life After Ablation
When should I go to the ER instead of calling my doctor
Go to urgent care or the ER if you have severe chest pain, fainting, major shortness of breath, new severe weakness, or symptoms that feel intense and escalating. If your wearable shows something concerning and you also feel very unwell, trust the whole picture, not just the app screen.
Call your doctor for non-emergency palpitations, repeated but stable symptoms, questions about medication, or ECG recordings that seem abnormal but aren't causing severe distress.
If you are unsafe, struggling to breathe, passing out, or having chest pain, don't wait for a portal message reply.
Can I exercise after ablation
A return to activity is generally possible, but the exact pace depends on the instructions from their own team. Start where your doctor told you to start. If movement reliably triggers symptoms, document that pattern and share it. Gentle return is different from pushing through severe symptoms.
Can lifestyle changes actually lower the chance of recurrence
Yes, and this is one of the most encouraging aspects of recovery. A Cleveland Clinic Journal of Medicine review reports that in patients with MASLD, losing 10% or more of body weight after ablation was associated with a 100% prevention rate, while 91% of those who gained weight had recurrent arrhythmia. The same review states that 100% of patients with rising HbA1c redeveloped AFib, as described in this Cleveland Clinic Journal of Medicine review on AF recurrence risk factors.
Those are striking findings. They don't mean weight or glucose are the only factors. They do mean daily habits can have real rhythm consequences.
Not sure what your ECG is showing? Qaly gets your recordings reviewed by human experts.



.png)
.png)