


Key Takeaways

User Profile
Hello Heart Hero.
You might be reading this because something felt wrong. Maybe it was a sharp pain in the center of your chest. Maybe it got worse when you took a deep breath, and then your mind went straight to the worst-case scenario. You checked your Apple Watch or Kardia, stared at the tracing, and hoped your device would tell you something clear.
That reaction makes sense.
Chest pain is scary, and many people feel stuck between two unsatisfying options. One is to panic and rush to the ER for every strange sensation. The other is to be told it's probably nothing, without anyone really explaining what your body might be doing. If you've felt skeptical of that gap, you're not overreacting. You're trying to understand your own heart.
That Sharp Chest Pain and Your Heart's Story
A common story goes like this. Someone feels a sudden chest pain that is sharper than expected, not the heavy pressure they imagined a serious heart problem would feel like. They sit down, breathe shallowly, maybe lean forward without even realizing it. Then they open their wearable ECG app and look for clues.
Pericarditis can fit that story.
Pericarditis means inflammation of the lining around the heart. It's considered a rare disease in the United States, with an estimated prevalence of around 160,000 individuals, yet it still accounts for up to 5% of emergency department visits for non-ischemic chest pain according to this PubMed review of US pericarditis prevalence. In plain English, that means it isn't common across the whole population, but it shows up often enough in chest pain evaluations that doctors take it seriously.
That mix is what makes it confusing. Rare enough that many people have never heard of it. Common enough in chest pain workups that it can absolutely be the answer.
Chest pain doesn't have to be dramatic to be real, and it doesn't have to be a heart attack to deserve attention.
Pericarditis is not a catch-all label for unexplained symptoms. It's a specific condition with patterns. There are symptoms that tend to go with it. There are ECG changes that can support it. There are warning signs that mean you shouldn't wait. There are also many cases that improve with treatment and careful follow-up.
If your wearable has picked up something odd, or if your symptoms keep coming back and nobody has connected the dots, knowledge helps. Not because you should diagnose yourself from a watch tracing, but because understanding the pattern can lower panic and help you seek the right level of care.
Why this can feel so unsettling
People often get thrown off by three things:
- The pain feels unusual: It can be sharp instead of crushing.
- The ECG may look subtle: Consumer devices can show hints, but not the whole picture.
- The cause may stay unclear: That uncertainty can make you feel like your concerns were dismissed.
None of that means you're imagining it. It means pericarditis lives in the gray zone where symptoms, timing, and smart interpretation matter.
What Is Pericarditis and Why Does It Happen
Think of your heart as wearing a thin, two-layered jacket. That jacket is called the pericardium. It helps protect the heart and lets it move smoothly as it beats. When that lining gets irritated and inflamed, the layers can rub against each other. That rubbing is one reason pericarditis can hurt.
The basic forms
Doctors usually describe pericarditis by its timing:
- Acute pericarditis: A newer episode that starts over hours, days, or a short period of time.
- Recurrent pericarditis: Symptoms go away, then later come back in separate flares.
- Chronic pericarditis: Inflammation or related problems last longer and can become more complicated.
For a patient, the timing matters because a one-time flare feels different from a pattern that keeps returning and disrupting daily life.
Why it happens
Many people want one neat answer for the cause. Sometimes there is one. Often there isn't.
A viral infection is a common trigger, but the exact cause often can't be identified, leading to what doctors call idiopathic pericarditis, as explained in this Harvard Health overview of pericarditis. That word can sound frustrating. It means "we don't have a confirmed specific cause," not "nothing is wrong" and not "someone missed something obvious."
Some people have underlying autoimmune conditions such as lupus or rheumatoid arthritis, where the immune system can mistakenly inflame the pericardium. In other cases, the trigger may relate to a recent illness, immune activation, injury, or another inflammatory process in the body. If you're trying to understand how body-wide inflammation can affect symptoms over time, this overview of chronic inflammation gives helpful context.
Practical rule: "Idiopathic" is not a shrug. It's a standard medical category when a clear trigger isn't found.
That matters because many patients interpret "unknown cause" as "nobody believes me." Those are not the same thing.
What often confuses people
Two things can be true at once. Pericarditis can be very uncomfortable, and many cases are still manageable. It can also be hard to pin down at first, especially if symptoms overlap with reflux, muscle strain, viral illness, or anxiety.
That's why a calm, pattern-based approach helps. What does the pain feel like? Does body position change it? Did symptoms begin after an illness? Is there a fever? Did the ECG change over time? Those details matter more than one isolated moment of fear.
Recognizing the Classic Signs of Pericarditis
Pericarditis has a "feel" that is often different from other causes of chest discomfort. The classic symptom is sharp chest pain. People may describe it as stabbing, catching, or painful enough that they instinctively avoid a deep breath.

The pain pattern that raises suspicion
One of the most useful clues is that the pain is often pleuritic, which means it worsens when you take a full breath, cough, or sometimes swallow. Another classic feature is position. Many people feel worse lying flat and better sitting up or leaning forward.
That positional pattern is important. It doesn't prove pericarditis by itself, but it gives doctors a strong clue because not all chest pain behaves that way.
Here are the symptoms patients often notice together:
- Sharp central chest pain: Usually under the breastbone, though it can spread toward the neck, shoulders, or upper back.
- Pain with deep breaths or coughing: This makes the discomfort feel especially alarming because each breath seems to trigger it.
- Relief when leaning forward: Many people discover this before they know it has a name.
- A generally sick feeling: Some people also notice fatigue, low energy, or fever.
What your body may be trying to tell you
If the inflamed lining also causes fluid to build up around the heart, symptoms can shift. Instead of just pain, someone might notice increasing breathlessness, a racing heart, or pressure that feels different from the earlier sharp pain.
If your pain changes from "sharp when I move or breathe" to "I feel short of breath, weak, or lightheaded," that deserves prompt medical attention.
Another place people get confused is palpitations. Pericarditis pain can make you tense, breathe differently, and feel every heartbeat. That doesn't always mean an arrhythmia is happening. But it also doesn't mean you should ignore rhythm symptoms, especially if your wearable captures an ECG during the episode.
A simple way to describe your symptoms clearly
If you talk to a clinician, urgent care team, or ECG reviewer, skip vague phrases like "my chest just felt weird." Try this instead:
- Where it is: center, left side, or spreading to neck or shoulder
- What it feels like: sharp, stabbing, burning, pressure, fluttering
- What changes it: deep breath, cough, lying down, leaning forward, walking
- What came with it: fever, shortness of breath, palpitations, dizziness
That kind of description makes the conversation more useful and often gets you taken more seriously.
Decoding Pericarditis on Your Wearable ECG
When pericarditis shows up on an ECG, it doesn't usually announce itself in a way that is obvious to a casual reader. That's especially true on a single-lead device like an Apple Watch or handheld monitor. Still, there are patterns worth understanding.
The classic ECG pattern
A key ECG finding in acute pericarditis is widespread concave ST elevation with PR depression, and a helpful clue is the ST/T wave ratio in lead V6. If the ST height divided by the T wave height is greater than 0.25, that strongly suggests pericarditis over benign early repolarization, according to this LITFL review of pericarditis ECG changes.
That sentence contains a lot of jargon, so let's translate it.
- ST elevation means part of the ECG tracing sits higher than expected.
- Concave means it curves upward in a smooth, scooped way rather than looking sharply peaked.
- PR depression is a subtler lowering of another part of the tracing.
- Widespread means it appears across multiple ECG leads, which is one reason a full 12-lead ECG is so helpful.
A single-lead wearable usually can't show the full "widespread" picture. That's the limitation. But it may still capture hints such as rhythm changes, heart rate trends, or evolving subtle shape changes that deserve closer review.
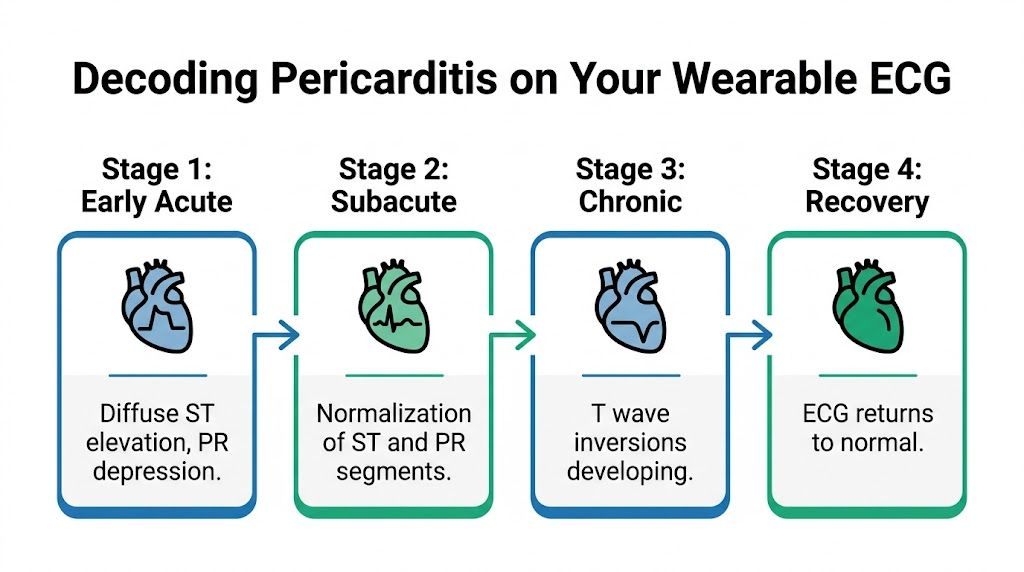
The four stages in simpler language
Pericarditis can move through a sequence on ECG:
- Early acute stage
ST segments rise and PR segments may dip. This is the phase people most often mean when they talk about "classic" pericarditis ECG changes. - Subacute stage
Those early changes begin to normalize. - Later stage
T waves may invert. This can confuse people because the tracing now looks different from the early stage. - Recovery
The ECG can return toward a more normal appearance.
These stages don't always show up neatly on a wearable. A watch gives you a narrow window. That's useful, but it isn't the same as standing in front of a full-length mirror.
A normal-looking single-lead wearable ECG doesn't rule out pericarditis, and an unusual-looking one doesn't confirm it by itself.



What your wearable can actually help with
Wearables are best used as timing tools and trend tools.
They can help you document:
- When symptoms happen: during rest, after illness, at night, after lying down
- Whether the rhythm stayed regular: useful if palpitations are part of the picture
- Whether the heart rate is persistently high: especially when symptoms are active
- Whether repeated tracings look different over time: serial recordings can matter more than one isolated strip
If you're using an Apple Watch and want a clearer sense of what a consumer device can and can't capture, this guide to ECG for Apple Watch is a good primer.
Why expert review matters
The most important ECG clues in pericarditis can be subtle. A machine may label a tracing "normal" or "inconclusive" when a trained human sees a pattern that fits the story better. The opposite can also happen. A strange-looking tracing may be a harmless variation, artifact, or lead placement issue rather than inflammation.
That's why context matters. ECG shape, symptom timing, body position, recent illness, and whether the tracing changed over days all help separate signal from noise.
Is It Pericarditis or Something Else
The hardest moment for many people is not the pain itself. It's the question behind it. "Is this pericarditis, or is this a heart attack?"
That fear is understandable, because several conditions can cause chest pain and some are urgent.
How the pain can differ
Pericarditis often causes sharp, breath-related, positional pain. Many people feel worse lying down and better leaning forward. A heart attack more often causes a pressure-like or squeezing discomfort that may spread to the arm, jaw, or back and is less tied to breathing or position.
GERD, or acid reflux, can burn and rise into the throat, often after meals or when lying down. Anxiety can create chest tightness, a racing heart, tingling, and a feeling of not getting enough air. A blood clot in the lung can also cause sharp chest pain, especially with breathing, but often comes with sudden shortness of breath and a different clinical story.
Here is the tricky part. Real life does not always read like a textbook.
Some people with serious heart problems don't feel "classic" pressure, and some people with pericarditis feel more than just sharp pain. That's why chest pain should never be reduced to one internet checklist.
Why doctors compare several possibilities
When clinicians evaluate chest pain, they aren't trying to be vague or dismissive by mentioning multiple causes. They're trying to sort dangerous conditions from less dangerous ones, and they often need ECGs, blood work, a physical exam, and sometimes imaging to do it safely.
Pericarditis can overlap with myocarditis, which involves inflammation of the heart muscle itself. If you've wondered how those conditions relate, this patient-friendly overview of myocarditis helps explain the distinction.
A calmer way to think about uncertainty
If your symptoms fit pericarditis, that can be reassuring in one sense because the pattern is recognizable and often treatable. But it shouldn't lead to self-diagnosis. The goal is not to talk yourself out of evaluation. The goal is to describe what you're feeling more precisely so the right evaluation happens sooner.
A helpful mindset is this:
- Don't panic over every chest sensation
- Don't dismiss sharp or recurring chest pain
- Do pay attention to pattern, timing, and associated symptoms
- Do get urgent help if symptoms are severe, new, or accompanied by shortness of breath, fainting, or collapse
That middle ground is where good decisions happen.
How Pericarditis Is Treated and When It Is an Emergency
Once pericarditis is diagnosed, treatment usually focuses on calming inflammation and preventing it from coming back. Many people are treated outside the hospital with anti-inflammatory medication. Common first-line treatment often includes an NSAID such as ibuprofen, along with colchicine, depending on the clinical situation.

What treatment is trying to accomplish
The goal isn't just pain relief. Doctors want to reduce the inflammation enough that the pericardium settles down and the chance of recurrence drops. That usually means taking medication exactly as directed and not stopping early just because the pain fades.
Rest matters too. If you're dealing with chest pain, palpitations, or ongoing inflammation, pushing through intense exercise can muddy the picture and make recovery harder.
When it stops being a "wait and see" problem
Most cases are managed as an outpatient, but some features raise concern. According to this AAFP summary of pericarditis risk features, hospitalization is more likely to be needed when there is a high fever over 38°C or 100.4°F, a large fluid collection around the heart, a subacute onset, or failure to respond to NSAID therapy after one week.
Those are clinical markers, but you can translate them into everyday warning signs.
Seek urgent or emergency care if you have:
- Severe shortness of breath: especially if it is getting worse or happens at rest
- Fainting or near-fainting: this can signal reduced blood flow or another serious problem
- A sense of pressure, collapse, or marked weakness: not just pain, but feeling medically unwell
- Persistent chest pain that is new or escalating: especially if you can't tell whether it could be a heart attack
- Fever with chest pain: particularly when symptoms are ongoing rather than improving
If your clinicians are checking for a heart attack, you may hear about blood tests such as troponin. This explainer on heart attack blood testing can make that part of the workup less mysterious.
The emergency complication people worry about
One dangerous complication is cardiac tamponade, which happens when fluid around the heart builds up enough to interfere with filling. You are not expected to diagnose that at home. What matters is recognizing the red flags that could point toward it, such as worsening breathlessness, lightheadedness, feeling faint, or a rapid decline in how you feel.
When to act fast: If chest pain is paired with trouble breathing, faintness, or a feeling that something is rapidly worsening, don't sit at home trying to interpret your watch. Get medical care.
A good rule is simple. If you are debating whether symptoms are "bad enough," but you feel unstable, that debate itself is the answer. Get evaluated.
Monitoring Your Heart Health After Pericarditis
Recovery doesn't always end when the first chest pain episode ends. One reason pericarditis creates so much anxiety is that it can come back after a period of feeling normal. Recurrent pericarditis affects 15% to 30% of patients, and episodes are sometimes missed because symptoms get partly masked by medications or mistaken for something else, as described by the American Heart Association page on recurrent pericarditis.
That can be maddening. You feel something real, but it's intermittent. By the time you get seen, the flare may have eased.
What good monitoring looks like
Wearables can be reassuring. Not because they replace medical care, but because they help you capture what was happening when symptoms were active.
A useful routine often includes:
- Recording an ECG when symptoms start
- Repeating it if the sensation changes
- Keeping brief notes about pain, position, fever, and palpitations
- Saving reports to share with your clinician
If your doctor orders imaging, this overview of a transthoracic echocardiogram can help you understand why an echo is often part of the follow-up.
Peace of mind comes from pattern, not guessing
The biggest benefit of monitoring is not constant checking for danger. It's reducing guesswork. Over time, a symptom diary plus wearable ECGs can show whether "random chest feelings" follow a recognizable pattern.
That doesn't solve everything, but it gives you something solid. And when you're dealing with a condition that can be painful, confusing, and occasionally recurrent, solid information is calming.
Tired of guessing what your ECG means? Let Qaly's experts review your recordings, track your intervals, and give you reports worth sharing with your doctor.



.png)
.png)