


Key Takeaways

User Profile
Hello Heart Hero. If you're reading this after seeing “mitral valve prolapse” on a test result, hearing a murmur, or noticing palpitations on your Apple Watch, Fitbit, or Kardia device, you're probably trying to connect pieces that don't seem to talk to each other. One part of the system gives you an echocardiogram report full of technical words. Another part gives you rhythm alerts, skipped beats, or tracings on your phone. It can feel like you're expected to make sense of both on your own.
That frustration is understandable. A lot of people want straight answers, not vague reassurance. They want to know what the mitral valve prolapse echocardiogram shows, what matters on the report, and whether their symptoms and wearable data fit the picture.
The good news is that these tools answer different questions. The echocardiogram looks at structure. Your wearable ECG looks at rhythm. When you understand how those two fit together, your situation often becomes much less mysterious.
Your Guide to Understanding an MVP Diagnosis
Mitral valve prolapse, often shortened to MVP, means the mitral valve doesn't move in the usual tidy way when the heart squeezes. The mitral valve sits between two chambers on the left side of the heart and acts like a one-way door. In MVP, one or both valve leaflets bow backward a bit during contraction.
That sentence sounds bigger than it is. For many people, MVP is something doctors monitor rather than something that takes over daily life. Still, hearing you have a valve issue can trigger anxiety fast, especially if you've also felt flutters, chest awareness, or odd beats that no one has clearly explained.
A useful starting point is remembering that MVP belongs under the broader umbrella of valvular heart disease. That doesn't automatically mean severe disease. It means the valve's shape or function deserves a closer look.
Why people get confused
Part of the confusion comes from how MVP is discussed. Some clinicians focus on the anatomy. Patients usually focus on how they feel. Wearables add a third layer by showing electrical activity that may or may not line up with symptoms in the moment.
A diagnosis is information, not a sentence.
The goal is to translate the report into everyday language. Once the medical wording becomes clear, you can ask better questions, notice more useful patterns, and walk into appointments with a lot more confidence.
What helps most
A simple way to think about this is:
- The echo shows the valve itself
- Your symptoms show your lived experience
- Your wearable ECG may capture what your heart rhythm was doing at that time
Put together, those pieces tell a fuller story than any one test can alone.
What an Echocardiogram Is and Why It Is Used for MVP
An echocardiogram, or echo, is an ultrasound of the heart. It uses sound waves to create moving images of your heart's chambers, valves, and blood flow. If you've ever seen an ultrasound in pregnancy care, the basic idea is similar. Different body part, same general technology.
For MVP, this matters because a doctor can't reliably diagnose the valve's motion by symptoms alone. Palpitations can come from many causes. Chest sensations can be misleading. An echo lets the team watch the mitral valve open and close beat by beat.
Think of it like sonar
A helpful analogy is sonar. The probe sends out sound waves, those waves bounce off heart structures, and the machine turns the returning signals into a live picture. That's why the test can show motion, not just a still snapshot.
This was a big step forward for MVP. Modern reviews note that MVP affects 2% to 3% of the population, which is more than 176 million people worldwide, and that echocardiography was the tool that established MVP as a true structural heart disorder rather than a vague label from older, less specific methods that once pushed estimates as high as 35% (European Heart Journal - Cardiovascular Imaging review).
What your clinician is looking for
During a mitral valve prolapse echocardiogram, the reader studies several things at once:
- Valve movement: whether one or both leaflets bow backward during contraction
- Valve appearance: whether the leaflets look thin, thickened, or redundant
- Blood flow: whether blood leaks backward through the valve
- Overall heart response: whether the nearby chambers seem to be handling things comfortably
That last part matters because a valve finding never exists in isolation. The report isn't just naming a valve shape. It's asking whether that shape is affecting blood flow or the workload on the heart.
The echocardiogram turns an invisible worry into something visible and measurable.
For many anxious patients, that's the moment things start feeling more solid. You move from “something might be wrong” to “this is what the valve is doing.”
Decoding Your Echocardiogram Report for MVP
Echo reports can look like they were written for another species. The trick is to pull out the few phrases that are key to the diagnosis. Once you know those, the report starts reading less like a code sheet and more like a description.
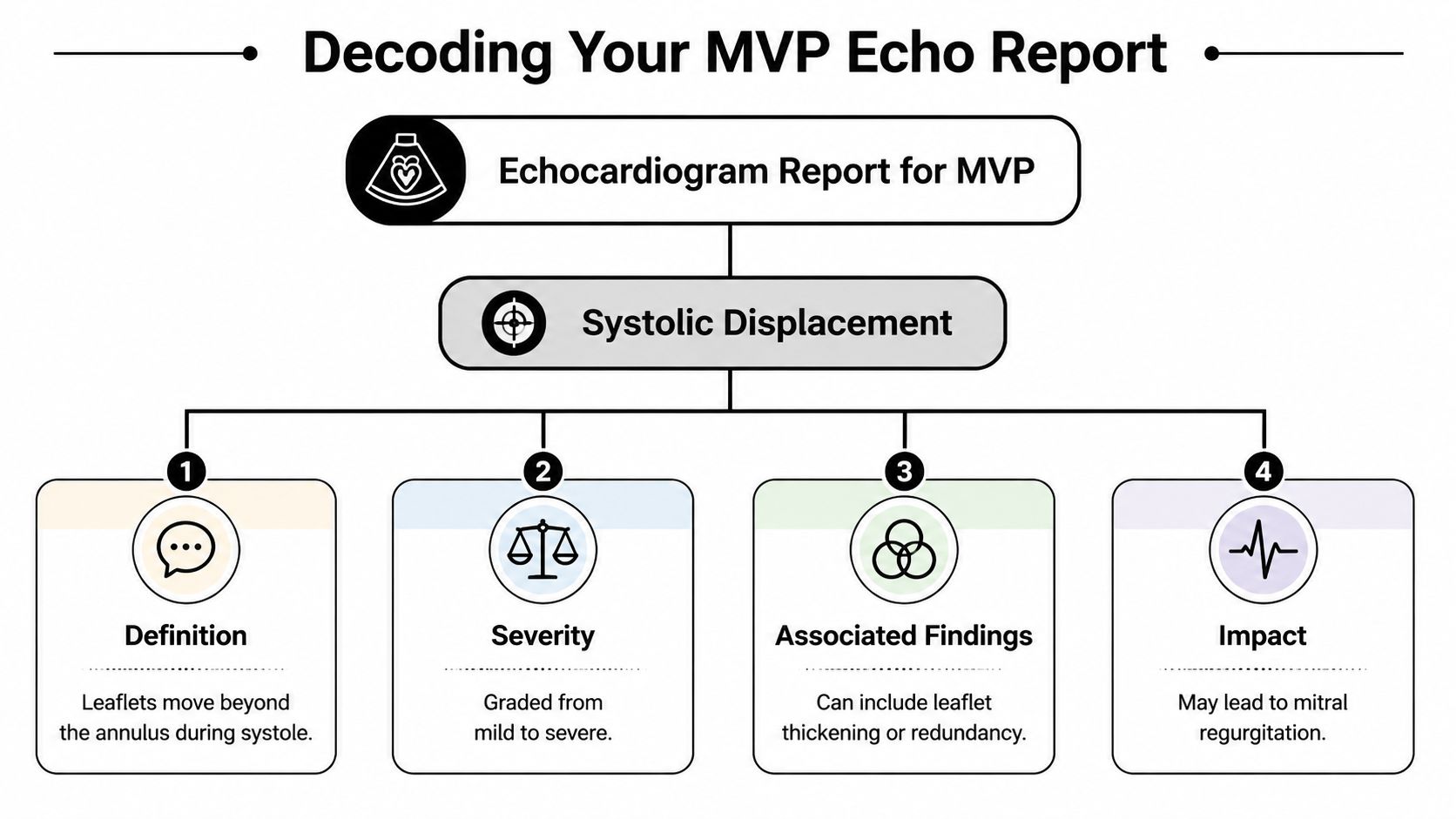
The key phrase is systolic displacement
The main diagnostic sign is systolic displacement. That means that when the heart squeezes, one or both mitral valve leaflets move backward above the annulus instead of staying neatly aligned.
The formal imaging criterion for MVP is systolic displacement of one or both mitral leaflets by more than 2 mm above the plane of the mitral annulus in a long-axis view (European Society of Cardiology imaging overview).
If your report says “prolapse” but doesn't explain it, that's the core idea hiding underneath the terminology.
Terms that often worry people
A few words tend to jump off the page:
- Leaflet means one of the valve flaps. The mitral valve has two.
- Annulus means the ring-like base where the valve sits.
- Thickened leaflets means the tissue looks bulkier than usual.
- Myxomatous usually means the valve tissue looks more floppy or redundant than normal.
“Myxomatous” is one of those words that sounds frightening because it's unfamiliar. In this setting, it's describing texture and shape, not delivering a dramatic verdict.
Why the report includes extra details
A good MVP echo report usually does more than say yes or no. Modern imaging reviews emphasize looking at leaflet length and thickness, prolapse distance, annular size, and whether the valve pattern involves one leaflet or both. Those details help the clinician understand the valve's morphology and how closely it should be followed over time.
Here are the parts most worth circling when you read your report:
- Was MVP seen?
Look for a direct statement that one or both mitral leaflets prolapse. - Is there mitral regurgitation?
This means blood is leaking backward when the valve closes. - How do the leaflets look?
Words like thickened, redundant, bileaflet, or myxomatous describe the valve's structure. - Does the report mention the annulus?
This tells you whether the ring around the valve looks enlarged or otherwise notable.
Practical rule: if you can't tell whether the report is describing valve shape, valve leak, or both, ask your clinician to separate those two issues out loud.
That one question often clears up half the confusion.
What not to overread
It's easy to stare at every line item and assume each one is dangerous. Most of the time, the most important information is concentrated in the impression or summary. The long body of the report often contains technical observations used to support that summary.
So if your eyes glaze over, come back to these plain-language questions:
- Is MVP present?
- Is there a leak?
- If there is a leak, how significant is it?
- Does the doctor want follow-up imaging?
Those answers matter more than memorizing every term.
Understanding Different Types of Echocardiograms
Not every echo is the same experience, and that's another place people get thrown off. If one doctor says “you need an echo” and another says “we may need a TEE” or “3D imaging,” it can sound like the situation suddenly got more serious. Often, it means they want a clearer angle.
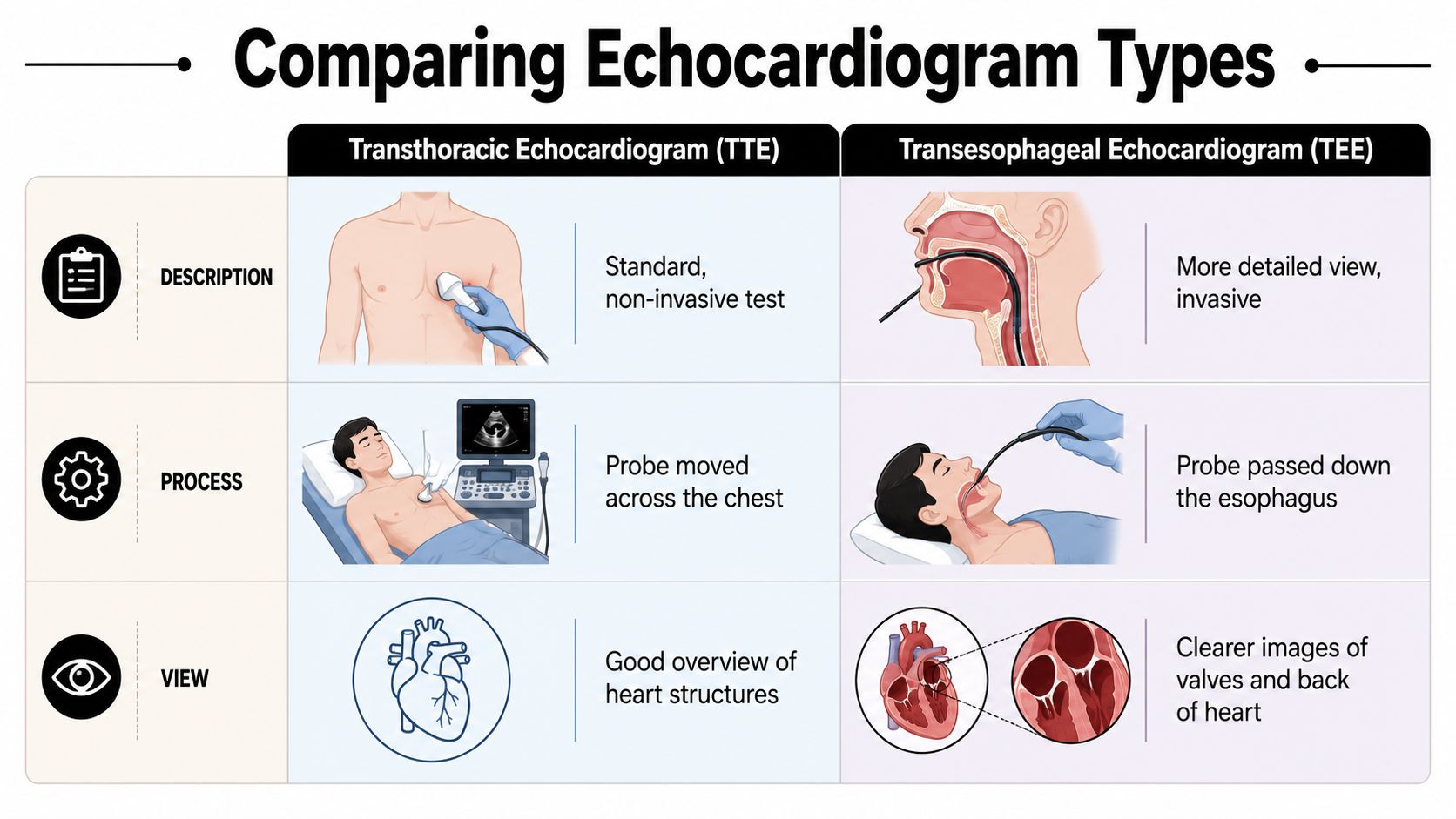
Transthoracic echo
The standard test is the transthoracic echocardiogram, or TTE. This is the one where a technician places gel on your chest and moves a probe across different spots to get pictures of the heart.
It is generally well tolerated. There's no radiation, no incision, and no recovery period. If you want a broader overview of how this standard ultrasound works, this guide to a transthoracic echocardiogram lays it out in plain language.
For MVP, TTE is usually the first step because it gives a strong overall view of the valve, heart chambers, and blood flow.



Transesophageal echo
A transesophageal echocardiogram, or TEE, gets the probe closer to the heart by placing it in the esophagus. Since the esophagus sits right behind the heart, the images can be much sharper for certain valve questions.
This is the one that sounds intimidating. That's normal. But the purpose is simple: reduce visual obstacles and get a cleaner look at the valve. It isn't ordered to scare you. It's ordered when detail matters.
3D echo
Then there's 3D echocardiography, which can be part of TTE or TEE imaging. Instead of flattening the valve into standard slices, it helps the team appreciate the valve as a three-dimensional structure.
A helpful analogy is the difference between reading a floor plan and walking through a room. Both are useful. One gives you a more intuitive sense of shape.
Why your doctor might choose one over another
A review on MVP imaging notes that 2D transthoracic Doppler echocardiography is the starting test, while 3D TTE and TEE are now routine for a complete assessment, especially for better detail on valve anatomy and the severity of any mitral regurgitation (PMC review on MVP imaging).
In plain language, that means:
- TTE is the front door
- TEE is the closer inspection
- 3D imaging helps define the valve's shape in more detail
If your doctor recommends a different type of echo after the first one, that doesn't automatically mean your condition worsened. It often means the first test raised a question that needs a sharper picture.
That distinction matters. Patients often hear “more testing” and assume “more danger.” In valve imaging, “more testing” often just means “more precision.”
Mitral Regurgitation Grading and What It Means
A lot of worry around MVP comes down to one related issue: mitral regurgitation. This means the valve lets some blood move backward when it should be closed.
The easiest analogy is a faucet. A tiny drip is different from a steady stream. Both count as leakage, but they don't mean the same thing.
How the grading works
Echo reports usually describe mitral regurgitation in simple categories such as:
- Mild
- Moderate
- Severe
Those categories matter because they help frame follow-up and treatment decisions. The valve prolapse itself is the structural finding. The regurgitation grade tells you how much that structure is affecting blood flow.
What those words usually mean in real life
Mild regurgitation usually means there is some leak, but not enough to create major concern on its own. In many cases, doctors watch it over time.
Moderate regurgitation sits in the middle. It often leads to closer follow-up, especially if symptoms, exam findings, or other echo features make the picture less straightforward.
Severe regurgitation is the category that gets the most attention because severe leaking is the pathway that can drive decisions about repair or replacement. In other words, it isn't the MVP label alone that usually leads to intervention. It's the impact of the leak.
If you want a patient-friendly explanation of what low-grade leaking often means, this article on mild valve regurgitation can help put the language in context.
The question to ask your doctor
Don't just ask, “Do I have regurgitation?” Ask, “How much, and are we watching for change?”
That second question is better because regurgitation is not an all-or-nothing issue. It lives on a spectrum, and your follow-up plan depends on where you are on that spectrum.
A leak on an echo report isn't automatically an emergency. The meaningful question is how significant it is and whether it's changing over time.
Connecting Echo Results to Your Symptoms and Wearable Data
Here, the hospital world and the everyday world finally meet.
An echo can tell you that the mitral valve prolapses and whether blood leaks backward. But it can't sit with you at work, in bed, after coffee, during stress, or on a walk when your heart suddenly feels like it's flipping, pausing, or fluttering. That's where wearable ECG devices come in.
Structure and rhythm are different questions
This distinction helps a lot:
- Your echocardiogram asks: What does the valve look like, and how is blood moving?
- Your wearable ECG asks: What electrical rhythm happened when I felt that symptom?
Those aren't competing tools. They're complementary tools.
If you feel a sudden thump or flutter, your Apple Watch, Fitbit, Kardia, Samsung watch, or similar device may catch the rhythm in that moment. That can help you and your clinician connect symptoms to actual electrical events instead of guessing from memory later.
Why wearables matter between appointments
Individuals often don't have symptoms while lying on an echo table. Symptoms show up in ordinary life. That's why many skeptical patients feel frustrated by the gap between “the test looked fine” and “I still feel something strange.”
A wearable helps narrow that gap. You can log when the symptom happened, what you were doing, whether it followed caffeine, stress, poor sleep, exercise, or nothing obvious at all. Over time, patterns may become easier to recognize.
If you're trying to make sense of recurring episodes over time, continuous monitoring in plain language is a useful concept to understand, even if your device only records on demand or in short windows.
Putting the two together
Here's the practical value of combining these worlds:
- The echo gives context
It tells you whether MVP is present and whether there is associated valve leakage. - The wearable captures moments
It may record what your rhythm was doing during a flutter, skipped beat sensation, or racing episode. - Your symptom notes add the human layer
They show how often this happens, how long it lasts, and what seems to trigger it.
One option some wearable users use is Qaly, which reviews wearable and at-home ECG recordings from devices like Apple Watch, Fitbit, and Kardia and provides technician-reviewed rhythm feedback. That's useful for people who want help interpreting recordings between office visits without relying only on auto-generated device labels.
Your body is giving you information all the time. The trick is organizing it so your clinician can use it.
When patients bring an echo report, symptom timeline, and wearable tracings together, appointments often become more productive. Instead of saying “I feel weird sometimes,” you can say, “Here is what the valve looks like, here is when the symptoms happen, and here is what my rhythm recording showed during one of those episodes.”
That's a much stronger position to be in.
Your Path Forward After an MVP Diagnosis
An MVP diagnosis usually isn't the end of a story. It's the start of a clearer one.
For many people, the next step is simple follow-up. That may mean repeat echocardiograms over time, paying attention to symptoms, and checking in sooner if something changes. What matters most is not panic. It's consistency.
A way to move forward
Keep your plan practical:
- Know your baseline: save a copy of your echo report and learn the key terms in it.
- Track symptoms: note when palpitations, chest awareness, shortness of breath, or fatigue show up.
- Bring your own data: wearable ECG recordings can make appointments much more concrete.
- Ask direct questions: especially about regurgitation severity and follow-up timing.
You don't need to become your own cardiologist. But you do deserve to understand what your tests mean, what your body is telling you, and what to watch next. That's not being difficult. That's being informed.
Confused by your wearable ECG? Get a human-reviewed interpretation from Qaly.



.png)
.png)